Interventional radiology
Diagnostic IR procedures are those intended to help make a diagnosis or guide further medical treatment, and include image-guided biopsy of a tumor or injection of an imaging contrast agent into a hollow structure, such as a blood vessel or a duct.
By contrast, therapeutic IR procedures provide direct treatment—they include catheter-based medicine delivery, medical device placement (e.g., stents), and angioplasty of narrowed structures.
[2] Vascular Biliary intervention[11] Catheter placement Ablative[13][14] Genitourinary[16] The treatment of gastrointestinal hemorrhage can range anywhere from monitoring an asymptomatic bleed to supporting and maintaining the hemodynamic function of the patient.
For most cases, collaboration between the gastroenterologist and interventional radiologist optimizes patient outcome but again, is largely dictated by anatomical location of the GI bleed.
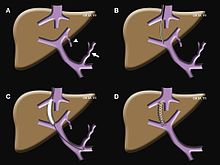
The portal vein is the site where hypertension (high blood pressure) can produce a myriad of deleterious effects throughout the liver and small or large intestine.
[19] Primarily, a TIPS functions to alleviate two different conditions: an emergent/life-threatening GI bleed or ascites (excessive abdominal fluid) caused by too high of blood pressure in the portal vein that is otherwise uncontrolled by diet and medications.
Depending on a patient's condition, this type of obstructive jaundice can be alleviated with surgery or chemotherapy but if these measures fail to restore proper flow of bile, an interventional radiologist can perform a procedure called a percutaneous transhepatic cholangiography (PTC).
[20] A PTC is an outpatient procedure lasting anywhere from 15 minutes to an hour where an interventional radiologist accesses the patient's bile duct system with a needle through the skin and liver under imaging guidance.
The prostate gland enlarges and compresses the adjacent urethra, making it difficult for men to control frequency and/or urgency of urination.
[22] Data suggests that TURP may have higher rates of symptom resolution at one and six months, but PAE appears to provide lower risks of complications more commonly associated with surgery, such as infection.
[28] A clot-busting medication such as tissue plasminogen activator (t-PA) can be used in a controlled hospital setting to dissolve the clot and help restore blood flow to the damaged area of the brain.
[29] Endovascular therapy is a procedure performed by neurointerventionalists to remove or dissolve the thrombus (clot) and restore blood flow to parts of the brain.
[32] During this treatment, an interventional radiologist inserts a catheter into the patient's leg and uses it to guide a coil through blood vessels to the site of the aneurysm.
[33] Imaging studies (DSA, CTA, or MRA) help characterize the aneurysm to decide the best course of treatment, whether endovascular coiling or surgical clipping.
[36] Endovascular embolization is a technique used by neurointerventionalists in which particles, glue, or coils are lodged inside the AVM to prevent blood flow through the abnormal channel.
A variety of interventional oncological treatments for tumors arise: Vascular disease refers to disorders of the vasculature or circulatory system, most commonly involving the arteries, veins and lymphatics.
Briefly, this involves using a needle to puncture a target vessel, then using a series of small medical guidewires and catheters to pass various tools inside for treatment.
Though numerous factors can affect patient's post-operative course, in general an endovascular approach is associated with a more rapid recovery time compared to a traditional open vascular surgery.
Medical management of atherosclerosis aims to address the many other known modifiable risk factors, such as smoking, diet, and exercise, as well as blood sugar levels in patients with diabetes.
When medical management fails, vascular interventional radiologists can attempt to restore blood flow to extremities using angioplasty and stenting.
Aneurysms can be solitary or multiple and are sometimes found in association with various clinical syndromes, including forms of vasculitis or connective tissue diseases.
Type B dissections begin in the distal aortic arch beyond the left subclavian artery origin, and may often be addressed with pain medication and blood pressure control.
If the type B aortic dissection results in poor circulation to the intestines, kidneys or legs it often requires urgent endovascular repair with endografts and/or fenestrations.
Carotid artery dissection, for example, places patients at increased risk for stroke and may extend further into the blood vessels within the brain.
Treatment of dissections depends on several factors, including the location, extent, how long it has been developing (acute or chronic) and whether it is limiting perfusion.
Interventional radiologists evaluate the blood supply of these patient's and may use balloons or stents to open narrowed vessels and keep the transplant organ functional.
Unlike arteries, veins are thin walled and distensible, allowing them to accommodate large volumes of blood without significant changes in pressure.
Interventional radiologists can use angiography to evaluate these structures (commonly called a istulogram) and treat dysfunctional access with angioplasty, stenting, and thrombectomy.
Dialysis catheters include temporary and tunneled large-bore central venous access lines placed for administering hemodialysis.
These lines differ in where they are inserted but are all placed under imaging guidance and adjusted so the end of the catheter sits in the vena cava adjacent to the heart.