Extraocular muscles
Precisely how the integration between voluntary and involuntary control of the eye occurs is a subject of continuing research.
The levator palpebrae superioris is responsible for raising the upper eyelid, and this can be a voluntary or involuntary action.
[5] The superior oblique muscle originates at the back of the orbit (a little closer to the medial rectus, though medial to it), getting rounder as it[5] courses forward to a rigid, cartilaginous pulley, called the trochlea, on the upper, nasal wall of the orbit.
The muscle becomes tendinous about 10mm before it passes through the pulley, turning sharply across the orbit, and inserts on the lateral, posterior part of the globe.
Due to its unique path, the superior oblique, when activated, pulls the eye downward and laterally.
In one eye, in two antagonistic muscles, like the lateral and medial recti, contraction of one leads to inhibition of the other.
[5] The extraocular muscles develop along with Tenon's capsule (part of the ligaments) and the fatty tissue of the eye socket (orbit).
This may be neurally coordinated by the central nervous system, to make the eyes move together and almost involuntarily.
This is a key factor in the study of strabismus, namely, the inability of the eyes to be directed to one point.
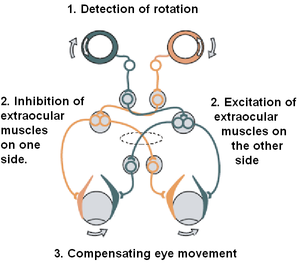
The reflex involves compensatory eye movements driven by inhibitory and excitatory signals.
[14] Damage to the oculomotor nerve (III) can cause double vision and inability to coordinate the movements of both eyes (strabismus), also eyelid drooping (ptosis) and pupil dilation (mydriasis).
[15] Lesions may also lead to inability to open the eye due to paralysis of the levator palpebrae muscle.
Individuals suffering from a lesion to the oculomotor nerve may compensate by tilting their heads to alleviate symptoms due to paralysis of one or more of the eye muscles it controls.
[14] Damage to the trochlear nerve (IV) can also cause double vision with the eye adducted and elevated.
When the eye is turned out (temporally) and horizontally, the function of the lateral rectus muscle is tested.
When the eye is turned in (nasally) and horizontally, the function of the medial rectus muscle is being tested.
To evaluate for weakness or imbalance of the muscles, a penlight is shone directly on the corneas.
Expected normal results of the corneal light reflex is when the penlight's reflection is located in the centre of both corneas, equally.