Misconceptions about HIV/AIDS
This myth has gained considerable notoriety as the perceived reason for certain sexual abuse and child molestation occurrences, including the rape of infants, in South Africa.
[14] Progress in testing methodology has enabled detection of viral genetic material, antigens, and the virus itself in bodily fluids and cells.
However, if the infected partner or both of the performers have blood in their mouth due to cuts, open sores, or gum disease, the risk increases.
In fact, disease progression can occur over a long period of time before the onset of symptoms, and as such, HIV infections cannot be detected based on appearance.
[29] On the other hand, a mosquito may have HIV-infected blood in its gut, and if swatted on the skin of a human who then scratches it, transmission is hypothetically possible,[30] though this risk is extremely small, and no cases have yet been identified through this route.
HIV can survive at room temperature outside the body for hours if dry (provided that initial concentrations are high),[31] and for weeks if wet (in used syringes/needles).
In the United States, the main route of infection is via homosexual anal sex, while for women transmission is primarily through heterosexual contact.
[34] HIV-infected women remain fertile, although in late stages of HIV disease a pregnant woman may have a higher risk of miscarriage.
Measles virus may persist for years in brain cells, eventually causing a chronic neurologic disease despite the presence of antibodies.
In other animals, viral relatives of HIV with long and variable latency periods, such as visna virus in sheep, cause central nervous system damage even after the production of antibodies.
[40] This "bystander killing" effect shows that great harm can be caused to the immune system even with a limited number of infected cells.
[41] In 1981 on June 5, the U.S. Centers for Disease Control and Prevention (CDC) published a Morbidity and Mortality Weekly Report (MMWR) describing cases of a rare lung infection, Pneumocystis carinii pneumonia (PCP), in five healthy gay men in Los Angeles.
However, high rates of mortality from these diseases, formerly confined to the elderly and malnourished, are now common among HIV-infected young and middle-aged people, including well-educated members of the middle class.
Because research in pathogenesis is difficult when precise animal models are unavailable, the disease-causing mechanisms in many diseases, including tuberculosis and hepatitis B, are poorly understood, but the pathogens responsible are very well established.
[3] The vast majority of people with AIDS never received antiretroviral drugs, including those in developed countries prior to the licensure of AZT in 1987.
[57] In the 1980s, clinical trials enrolling patients with AIDS found that AZT given as single-drug therapy conferred a survival advantage compared to placebo, albeit modest and short-lived.
Among HIV-infected patients who had not yet developed AIDS, placebo-controlled trials found that AZT given as a single-drug therapy delayed, for a year or two, the onset of AIDS-related illnesses.
In more recent years, three-drug combination therapies have produced another 50–80% improvements in progression to AIDS and in survival when compared to two-drug regimens in clinical trials.
[59][60][61][62][63][64][65][66][67][68][excessive citations] The proposed behavioral causes of AIDS, such as multiple sexual partners and long-term recreational drug use, have existed for many years.
The epidemic of AIDS, characterized by the occurrence of formerly rare opportunistic infections such as Pneumocystis carinii pneumonia (PCP), did not occur in the United States until a previously unknown human retrovirus—HIV—spread through certain communities.
For example, in a prospectively studied cohort in Vancouver, British Columbia, 715 homosexual men were followed for a median of 8.6 years.
[70] Other studies show that among homosexual men and injection-drug users, the specific immune deficit that leads to AIDS—a progressive and sustained loss of CD4+ T-cells—is extremely rare in the absence of other immunosuppressive conditions.
[71] In a survey of 229 HIV-seronegative injection-drug users in New York City, mean CD4+ T-cell counts of the group were consistently more than 1000 cells/μL of blood.
Only two individuals had two CD4+ T-cell measurements of less than 300/μL of blood, one of whom died with cardiac disease and non-Hodgkin's lymphoma listed as the cause of death.
[77] Among HIV-infected hemophiliacs, Transfusion Safety Study investigators found that neither the purity nor the amount of factor VIII therapy had a deleterious effect on CD4+ T-cell counts.
[78] Similarly, the Multicenter Hemophilia Cohort Study found no association between the cumulative dose of plasma concentrate and incidence of AIDS among HIV-infected hemophiliacs.
The median period of time between infection with HIV and the onset of clinically apparent disease is approximately 10 years in industrialized countries, according to prospective studies of homosexual men in which dates of seroconversion are known.
Similar estimates of asymptomatic periods have been made for HIV-infected blood-transfusion recipients, injection-drug users and adult hemophiliacs.
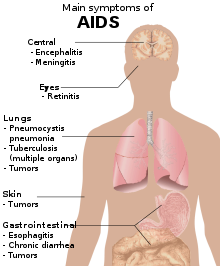
[38][85][86] Most AIDS symptoms result from the development of opportunistic infections and cancers associated with severe immunosuppression secondary to HIV.
As the immune system of an HIV-infected individual weakens, he or she becomes susceptible to the particular viral, fungal, and bacterial infections common in the community.