Hepatitis B
For others, symptoms may appear 30 to 180 days after becoming infected and can include a rapid onset of sickness with nausea, vomiting, yellowish skin, fatigue, yellow urine, and abdominal pain.
[4] In areas where the disease is common, infection around the time of birth or from contact with other people's blood during childhood are the most frequent methods by which hepatitis B is acquired.
[4] In areas where the disease is rare, intravenous drug use and sexual intercourse are the most frequent routes of infection.
[10] The hepatitis B viruses cannot be spread by holding hands, sharing eating utensils, kissing, hugging, coughing, sneezing, or breastfeeding.
[1] The World Health Organization (WHO) recommends infants receive the vaccine within 24 hours after birth when possible.
Using antiviral prophylaxis to prevent mother-to-child transmission is also recommended, as is following safe sex practices, including the use of condoms.
[20] Acute infection with hepatitis B virus is associated with acute viral hepatitis, an illness that begins with general ill-health, loss of appetite, nausea, vomiting, body aches, mild fever, and dark urine, and then progresses to development of jaundice.
[22][23] Chronic carriers are encouraged to avoid consuming alcohol as it increases their risk for cirrhosis and liver cancer.
[citation needed] Early life horizontal transmission can occur through bites, lesions, certain sanitary habits, or other contact with secretions or saliva containing HBV.
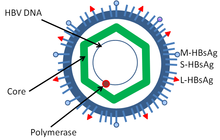
[41] In addition to the Dane particles, filamentous and spherical bodies lacking a core can be found in the serum of infected individuals.
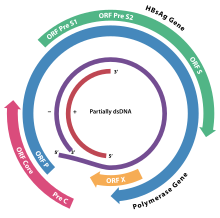
The HBsAg gene is one long open reading frame but contains three in frame "start" (ATG) codons that divide the gene into three sections, pre-S1, pre-S2, and S. Because of the multiple start codons, polypeptides of three different sizes called large (the order from surface to the inside: pre-S1, pre-S2, and S ), middle (pre-S2, S), and small (S)[46] are produced.
[47] There is a myristyl group, which plays an important role in infection, on the amino-terminal end of the preS1 part of the large (L) protein.
These four viral transcripts undergo additional processing and go on to form progeny virions that are released from the cell or returned to the nucleus and re-cycled to produce even more copies.
Differences between genotypes affect the disease severity, course and likelihood of complications, and response to treatment and possibly vaccination.
[51] There is evidence that the receptor in the closely related duck hepatitis B virus is carboxypeptidase D.[60][61] The virions bind to the host cell via the preS domain of the viral surface antigen and are subsequently internalized by endocytosis.
Traditionally, the presence of HBeAg in a host's serum is associated with much higher rates of viral replication and enhanced infectivity; however, variants of the hepatitis B virus do not produce the 'e' antigen, so this rule does not always hold true.
PCR tests have been developed to detect and measure the amount of HBV DNA, called the viral load, in clinical specimens.
[76] However, there is not sufficient evidence that the administration of hepatitis B immunoglobulin alone during pregnancy, might reduce transmission rates to the newborn infant.
[77] No randomized control trial has been conducted to assess the effects of hepatitis B vaccine during pregnancy for preventing infant infection.
[80] In assisted reproductive technology, sperm washing is not necessary for males with hepatitis B to prevent transmission, unless the female partner has not been effectively vaccinated.
[86][87] Early antiviral treatment may be required in fewer than 1% of people, whose infection takes a very aggressive course (fulminant hepatitis) or who are immunocompromised.
Chronically infected individuals with persistently elevated serum alanine aminotransferase, a marker of liver damage, and HBV DNA levels are candidates for therapy.
In 2010, the Hepatitis B Foundation reported that 3 preclinical and 11 clinical-stage drugs were under development, based on largely similar mechanisms.
More than 95% of people who become infected as adults or older children will stage a full recovery and develop protective immunity to the virus.
[92] Hepatitis B virus DNA remains in the body after infection, and in some people, including those that do not have detectable HBsAg, the disease recurs.
[105] Immunosuppressive drugs favor increased HBV replication while inhibiting cytotoxic T cell function in the liver.
[111][112] In moderate prevalence areas where 2–7% of the population is chronically infected, the disease is predominantly spread horizontally, often among children, but also vertically.
[122] Hepatitis B virus subgenotype C4 is exclusively present in Australian aborigines, suggesting an ancient origin as much as 50,000 years old.
Lurman's paper, now regarded as a classical example of an epidemiological study, proved that contaminated lymph was the source of the outbreak.
Later, numerous similar outbreaks were reported following the introduction, in 1909, of hypodermic needles that were used, and, more importantly, reused, for administering Salvarsan for the treatment of syphilis.




|
no data
<10
10–20
20–40
40–60
60–80
80–100
|
100–125
125–150
150–200
200–250
250–500
>500
|
