Dental extraction
Extractions are performed for a wide variety of reasons, but most commonly to remove teeth which have become unrestorable through tooth decay, periodontal disease, or dental trauma, especially when they are associated with toothache.
Extractions could be categorized into non-surgical (simple) and surgical, depending on the type of tooth to be removed and other factors.
[2] There are several techniques to achieve numbness of the tooth including The two most commonly used local anaesthetics in the UK are lidocaine and articaine.
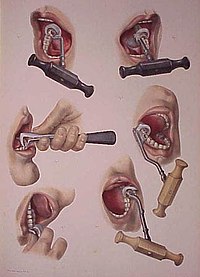
[2] During extraction, multiple instruments are used to aid and ease the removal of the tooth whilst trying to minimally traumatise the tissues to allow for quicker healing.
Using straw for drinking is also prohibited due to the negative pressure it can produce which will lead to removal of a newly formed clot from the socket.
[5] Bleeding of soft tissues can be controlled by several means including suturing the wound (stitches) and/ or using chemical agents such as tranexamic acid, ferric sulphate and silver nitrate.
Once the periodontal ligament is broken and the supporting alveolar bone has been adequately widened the tooth can be removed.
Common risks after any extraction include pain, swelling, bleeding, bruising, infection, trismus (not being able to open as wide as normal) and dry socket.
There are additional risks associated with the surgical extraction of wisdom teeth in particular: permanent or temporary damage to the inferior alveolar nerve +/- lingual nerve, causing permanent or temporary numbness, tingling or altered sensation to the lip, chin +/- tongue.
Historically, the anticoagulant warfarin (belonging to the group of drugs called coumarins) and antiplatelets such as aspirin or clopidogrel, were prescribed commonly in these circumstances.
There is evidence that use of antibiotics before and/or after impacted wisdom tooth extraction reduces the risk of infections by 66%, and lowers incidence of dry socket by one third.
Damage to the inferior alveolar nerve is a risk of lower wisdom tooth removal (and other surgical procedures in the mandible).
[20] This means there is a risk of temporary or permanent numbness or altered sensation to the lip +/- chin on the side the surgery is taking place.
Pressure is applied by the patient biting on a gauze swab, and a thrombus (blood clot) forms in the socket (hemostatic response).
Common hemostatic measures include local pressure application with gauze, and the use of oxidized cellulose (gelfoam) and fibrin sealant.
Dental practitioners usually have absorbent gauze, hemostatic packing material (oxidized cellulose, collagen sponge), and suture kit available.
Coagulopathies (clotting disorders, e.g. hemophilia) are sometimes discovered for the first time if a person has had no other surgical procedure in their life, but this is rare.
Bone remodeling as the alveolus adapts to the edentulous state occurs in the longer term as the alveolar process slowly resorbs.
Many drug therapies are available for pain management after third molar extractions including NSAIDS (non-steroidal anti-inflammatory), APAP (acetaminophen), and opioid formulations.
According to two doctors, Ibuprofen-APAP combinations have the greatest efficacy in pain relief and reducing inflammation along with the fewest adverse effects.
[37] Should post-extraction bleeding occur, UK guidance recommends biting onto a piece of damp gauze for at least 20 minutes whilst sitting in an upright position.
[28] It is important that the gauze is damp, but not soaking, to avoid disrupting clot formation and consequently inducing a rebound bleed.
If the socket continues to bleed, it is recommended to repeat the process with a fresh piece of damp gauze for 20 minutes again.
[41] In view of the lack of reliable evidence, clinicians must use their clinical experience to determine the most appropriate means of treating this condition, depending on patient-related factors.
[56] Techniques involve minimal use of forceps, which damage socket walls, relying instead on luxators, elevators and syndesmotomy.
The options to fill this gap are commonly recorded as Bind, and the choice is made by dentist and patient based on several factors.
[60] As dental extractions can vary tremendously in difficulty, depending on the patient and the tooth, a wide variety of instruments exist to address specific situations.