Hypokinesia
[11][12] Essential to the basal ganglionic-thalamocortical loop, which processes motor function, dopamine depletion is common in these areas of hypokinesic patients.
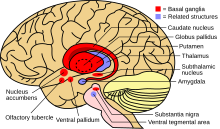
[12] The dopamine pathway in the substantia nigra is essential to motor function, and commonly a lesion in this area correlates with displayed hypokinesia.
[12][13] Tremor and rigidity, however, seem to be only partially due to dopamine deficits in the substantia nigra, suggesting other processes are involved in motor control.
[16] Hypokinetic symptoms arise from damage to the basal ganglia, which plays a role in producing force and computing the effort necessary to make a movement.
When activated, the direct pathway sends sensory and motor information from the cerebral cortex to the first structure of the basal ganglia, the putamen.
[18] Recent research indicates, when oscillations fire simultaneously, processing is disrupted at the thalamus and cortex, affecting activities such as motor planning and sequence learning, as well as causing hypokinetic tremors.
Physicians have experienced success treating this sleep disorder with slow-release or night-time dopaminergic drugs, and in some cases, continuous stimulation by the dopamine agonist rotigotine.
[19] Once the reaction to dopaminergic drugs begins to fluctuate in Parkinson's patients, deep brain stimulation (DBS) of the subthalamic nucleus and internal globus pallidus is often used to treat hypokinesia.
[21][22] Posteroventral pallidotomy (PVP) is a specific kind of DBS that destroys a small part of the globus pallidus by scarring the neural tissue, reducing brain activity and therefore tremors and rigidity.
This treatment has been shown to reduce hypokinesia in animal studies when increasing nociception FQ in the substantia nigra and subthalamic nucleus.
Low doses can be taken with dopaminergic treatment to decrease the amount of L-dopa needed, which can reduce its long-term side effects and improve motor performance.
[29] Dance therapy has also been shown to reduce hypokinesic movements and rigidity, though targeted more at the muscular aspects of the disorder than the neural activity.
[11] Tremor and rigidity have not had observable connections to cognitive impairments, supporting the idea that they are not as involved in the dopamine pathway in the basal ganglionic-thalamocortical loop.
[32] In fact, the motor planning and control of a patient with hypokinesia is already as efficient as possible (as shown by slightly faster, but generally the same movement after deep brain stimulation of the subthalamic nucleus).
[35] Gender More men than women typically develop hypokinesia, which is reflected in young and middle-aged populations where females have displayed higher levels of nigrostriatal dopamine than males.
In young-onset hypokinesia (younger than 45 years of age), typically slightly more cell loss occurs in the substantia nigra with more displayed dystonia and muscle stiffness.
Therefore, when a hypokinesia victim is under stress, he or she does not display a typical fight-or-flight response, placing the patient under greater danger from potentially harmful stimuli.