Health care reforms proposed during the Obama administration
His plan mentions: deficit neutrality; not allowing insurance companies to discriminate based on pre-existing conditions; capping out of pocket expenses; creation of an insurance exchange for individuals and small businesses; tax credits for individuals and small companies; independent commissions to identify fraud, waste and abuse; and malpractice reform projects, among other topics.
[12][13] In November 2009, then-OMB Director Peter Orszag described aspects of the Obama administration's strategy during an interview: "In order to help contain [ Medicare and Medicaid ] cost growth over the long term, we need a new health care system that has digitized information...in which that information is used to assess what’s working and what’s not more intelligently, and in which we’re paying for quality rather than quantity while also encouraging prevention and wellness."
[16] A report published by the Commonwealth Fund in December 2007 examined 15 federal policy options and concluded that, taken together, they had the potential to reduce future increases in health care spending by $1.5 trillion over the next 10 years.
The authors concluded that there are no magic bullets for controlling health care costs, and that a multifaceted approach will be needed to achieve meaningful progress.
The causes are disputed, ranging from recession-related delays in visiting doctors to more long-term trends in moderating insurance premiums and reduced spending on structures and equipment.
Washington Post columnist David Ignatius has also recommended that President Obama engage someone like Cortese to have a more active role in driving reform efforts.
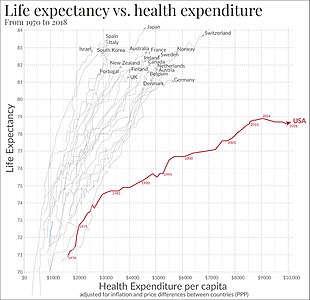
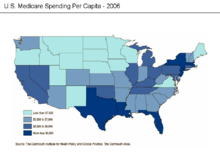
According to economist Peter A. Diamond and research cited by the Congressional Budget Office (CBO), the cost of healthcare per person in the U.S. also varies significantly by geography and medical center, with little or no statistical difference in outcome.
Two of these include:[58] Gawande argued: "Our fee-for-service system, doling out separate payments for everything and everyone involved in a patient’s care, has all the wrong incentives: it rewards doing more over doing right, it increases paperwork and the duplication of efforts, and it discourages clinicians from working together for the best possible results.
[68] A New York study found that only 1.5% of hospital negligence led to claims; moreover, the CBO observed that "health care providers are generally not exposed to the financial cost of their own malpractice risk because they carry liability insurance, and the premiums for that insurance do not reflect the records or practice styles of individual providers but more-general factors such as location and medical specialty.
Writing in The Washington Post, cardiologist Arthur Feldman cited various studies that indicate the U.S. is facing a "critical" shortage of doctors, including an estimated 1,300 general surgeons by 2010.
An amendment to the Senate health bill includes $2 billion in funds over 10 years to create 2,000 new residency training slots geared toward primary care medicine and general surgery.
[w]ithout appropriate adjustments, a simple cap may exacerbate rather than ameliorate current inequities"[90] Premium tax subsidies to help individuals purchase their own health insurance have also been suggested as a way to increase coverage rates.
[103] According to one study conducted by the Urban Institute, if not implemented on a systematic basis with appropriate safeguards, market reform has the potential to cause more problems than it solves.
These proposals generally exclude small firms, do not distinguish between individuals who have access to other forms of coverage and those who do not, and increase the overall compensation costs to employers.
[104] In October 2009 the Wall Street Journal reported that while requirements to purchase health insurance were central to proposals in both the House and Senate, these coverage mandates were "under fire from both ends of the political spectrum, with some liberals saying the penalties are too harsh for those who refuse and conservatives denouncing the whole concept.
"[107] She described the Massachusetts mandates as "a windfall for the insurance industry" and wrote, "Premiums are rising much faster than income, benefit packages are getting skimpier, and deductibles and co-payments are going up.
"[107] Addressing the issue when it was proposed in 1994, CBO wrote: "A mandate requiring all individuals to purchase health insurance would be an unprecedented form of federal action.
[113] President Barack Obama argues that U.S. healthcare is rationed, based on income, type of employment, and pre-existing medical conditions, with nearly 46 million uninsured.
[83][115] Former Republican Secretary of Commerce Peter G. Peterson has also argued that some form of rationing is inevitable and desirable considering the state of U.S. finances and the trillions of dollars of unfunded Medicare liabilities.
[118] Senator Charles Grassley (R-IA) makes similar arguments claiming for example that people like the late Senator Edward Kennedy received health care in the U.S. that would have been denied in countries which have government controlled health care,[119] a claim that The Economist magazine said was "dangerous" and went on to say that "The reality is that America, like Britain, already makes extensive use of rationing.
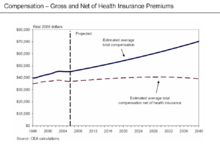
[133] In March 2010, billionaire Warren Buffett commented that the high costs paid by U.S. companies for their employees' health care put them at a competitive disadvantage.
[137] Even for those who are employed, the private insurance in the US varies greatly in its coverage; one study by the Commonwealth Fund published in Health Affairs estimated that 16 million U.S. adults were underinsured in 2003.
The underinsured were significantly more likely than those with adequate insurance to forgo health care, report financial stress because of medical bills, and experience coverage gaps for such items as prescription drugs.
[138] However, a study published by the Kaiser Family Foundation in 2008 found that the typical large employer preferred provider organization (PPO) plan in 2007 was more generous than either Medicare or the Federal Employees Health Benefits Program Standard Option.
This relates to moral arguments for health care reform, framing healthcare as a social good, one that is fundamentally immoral to deny to people based on economic status.
[145] The motivation behind healthcare reform in response to the medical-industrial complex also stems from issues of social inequity, promotion of medicine over preventative care.
[147] Likewise, critiques of insurance markets being conducted under a capitalistic, free-market model also include that medical solutions, as opposed to preventative healthcare measures, are promoted to maintain this medical-industrial complex.
[148][149][150] In December 2011 the outgoing Administrator of the Centers for Medicare & Medicaid Services, Donald Berwick, asserted that 20% to 30% of health care spending is waste.
[152] The International Federation of Health Plans provides a comparative annual survey of costs for drugs, devices and medical services across countries.
According to Bloomberg News, drugmakers agreed in June 2009 to contribute $80 billion over 10 years, largely to help the elderly afford medicines, in return for staving off other profit-endangering proposals such as drug importation.