Health effects of radon
Radon is a radioactive, colorless, odorless, tasteless noble gas, which has been studied by a number of scientific and medical bodies for its effects on health.
In every 1 square mile of surface soil, the first 6 inches (150 mm) (of depth) contains about 0.035 oz of radium (0.4 g per km2) which releases radon in small amounts to the atmosphere.
He was told that living in the home was the equivalent of smoking 135 packs of cigarettes a day, and he and his family had increased their risk of developing lung cancer by 13 or 14 percent.
Though at the time radon itself was not understood to be the cause—indeed, neither it nor radiation had even been discovered—mineralogist Georg Agricola recommended ventilation of mines to avoid this mountain sickness (Bergsucht).
[citation needed] The first major studies with radon and health occurred in the context of uranium mining, first in the Joachimsthal region of Bohemia and then in the Southwestern United States during the early Cold War.
In recent years, the average annual exposure of uranium miners has fallen to levels similar to the concentrations inhaled in some homes.
Smaller diameter particles diffuse further into the respiratory system, whereas the larger—tens to hundreds of micron-sized—particles often deposit higher in the airways and are cleared by the body's mucociliary staircase.
[1] While radon presents the aforementioned risks in adults, exposure in children leads to a unique set of health hazards that are still being researched.
[55] The resulting health effects in children are similar to those of adults, predominantly including lung cancer and respiratory illnesses such as asthma, bronchitis, and pneumonia.
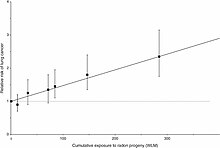
Studies of miners exposed to radon and its decay products provide a direct basis for assessing their lung cancer risk.
[citation needed] The ICPR 65 model[61] follows the same approach, and estimates the relative lifelong risk probability of radon-induced cancer death to 1.23 × 10−6 per Bq/(m3·year).
[62] In the absence of other causes of death, the absolute risks of lung cancer by age 75 at usual radon concentrations of 0, 100, and 400 Bq/m3 would be about 0.4%, 0.5%, and 0.7%, respectively, for lifelong nonsmokers, and about 25 times greater (10%, 12%, and 16%) for cigarette smokers.
[66] Although radon may present significant risks, thousands of persons annually go to radon-contaminated mines for deliberate exposure to help with the symptoms of arthritis without any serious health effects.
[citation needed] The study design for epidemiological methods may be of three kinds: Furthermore, theory and observation must confirm each other for a relationship to be accepted as fully proven.
Even when a statistical link between factor and effect appears significant, it must be backed by a theoretical explanation; and a theory is not accepted as factual unless confirmed by observations.
For that study, the odds ratio was found to be increased slightly above the confidence interval (95% CI) for cumulative radon exposures above 17 WLM (6.2 pC/L=230 Bq/m3 and above).
[citation needed] The results of a methodical ten-year-long, case-controlled study of residential radon exposure in Worcester County, Massachusetts, found an apparent 60% reduction in lung cancer risk amongst people exposed to low levels (0–150 Bq/m3) of radon gas; levels typically encountered in 90% of American homes—an apparent support for the idea of radiation hormesis.
[68] Radioactive water baths have been applied since 1906 in Jáchymov, Czech Republic, but even before radon discovery they were used in Bad Gastein, Austria.
In the United States and Europe there are several "radon spas", where people sit for minutes or hours in a high-radon atmosphere in the belief that low doses of radiation will invigorate or energize them.
The gold layer keeps the radon within, and filters out the alpha and beta radiation, while allowing the gamma rays to escape (which kill the diseased tissue).
In the radiobiology and carcinogenesis studies, progress has been made in understanding the first steps of cancer development, but not to the point of validating a reference dose-effect model.
[40] Given the radon distribution observed in dwellings, and the dose-effect relationship proposed by a given model, a theoretical number of victims can be calculated, and serve as a basis for public health policies.
[citation needed] With the BEIR VI model, the main health effect (nearly 75% of the death toll) is to be found at low radon concentration exposures, because most of the population (about 90%) lives in the 0–200 Bq/m3 range.
The linear no-threshold model has since been kept in a conservative approach by the UNSCEAR[41] report and the BEIR VI and BEIR VII[91] publications, essentially for lack of a better choice:Until the [...] uncertainties on low-dose response are resolved, the Committee believes that [the linear no-threshold model] is consistent with developing knowledge and that it remains, accordingly, the most scientifically defensible approximation of low-dose response.
[99] After publication of the North American and European Pooling Studies, Health Canada proposed a new guideline that lowers their action level from 800 to 200 Bq/m3 (22 to 5 pCi/L).
The United States Environmental Protection Agency (EPA) recommends homes be fixed if an occupant's long-term exposure will average 4 picocuries per liter (pCi/L) that is 148 Bq/m3.
Since air pressure is usually lower inside houses than it is outside, the home acts like a vacuum, drawing radon gas in through cracks in the foundation or other openings such as ventilation systems.
Radon levels in indoor air can be lowered in several ways, from sealing cracks in floors and walls to increasing the ventilation rate of the building.
To address the more common problem of breathing in radon released from water used during showers and other household activities, a point-of-entry solution may be more reliable.
[109] The high cost of radon remediation in the 1980s led to detractors arguing that the issue is a financial boondoggle reminiscent of the swine flu scare of 1976.

Pb is formed from the decay of 222
Rn . Here is a typical deposition rate of 210
Pb as observed in Japan as a function of time, due to variations in radon concentration. [ 4 ]