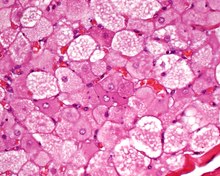
Hibernoma
They were first described under the name ‘pseudolipoma’ by the German physician H. Merkel in 1906 and the term hibernoma was proposed by the French anatomist Louis Gery in 1914 because of its resemblance to brown fat in hibernating animals.
[1][2][3] Patients present with a slow-growing, painless, solitary mass, usually of the subcutaneous tissues.
Serpentine, thin, low signal bands (septations or vessels) are often seen throughout the tumor.
The neoplastic cells are S100 protein positive (approximately 80%), and show membrane and vacuole CD31 immunoreactivity.
It is important to separate hiberoma from adult rhabdomyoma, a granular cell tumor and a true liposarcoma.
[4] Complete surgical excision is the treatment of choice, associated with an excellent long term clinical outcome.
In rare cases hibernoma may arise in bone tissue, however it is an incidental finding.