Human metapneumovirus
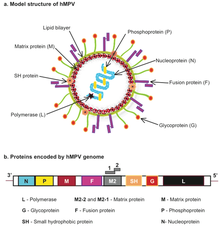
Human metapneumovirus (HMPV or hMPV) is a negative-sense single-stranded RNA virus of the family Pneumoviridae and is closely related to the avian metapneumovirus (AMPV) subgroup C. It was isolated for the first time in 2001 in the Netherlands by using the RAP-PCR (RNA arbitrarily primed PCR) technique for the identification of unknown viruses growing in cultured cells.
[4] When researchers began applying molecular biology techniques, the genetic characteristics and portions of the genomic sequences of the virus could be identified.
[27][28][29] Numerous outbreaks of HMPV have been reported in long-term care facilities for children and adults, causing fatalities.
[7] We see that proteins N, P, and L dissociate from the vRNA and bind to each other to form the polymerase complex so that the genomic RNA can act as a matrix for viral transcription and replication in the cytoplasm.
[37] The final step in the replication process of hMPV that is relatively certain is the journeying of the envelope glycoproteins (F, G, and SH) to zones of membranous accumulation via the Golgi apparatus to be exposed at the surface of infected cells.
HMPV is thought to attach to the target cell via the glycoprotein (G) protein interactions with heparan sulfate and other glycosaminoglycans.
[42][43] HMPV then induces the response of chemokines and cytokines such as IL-6, IFN-alpha, TNF-alpha, IL-2, and macrophage inflammatory proteins, which in turn leads to peribronchiolar and perivascular infiltration and inflammation.
[44] The identification of HMPV has predominantly relied on reverse-transcriptase polymerase chain reaction (RT-PCR) technology to amplify directly from RNA extracted from respiratory specimens.
[4] As of 2022[update], peak infection from hMPV in the northern hemisphere is in late winter and early spring, but it can be found globally across all continents[45] and its distribution is very complex and dynamic.
[4] This phenomenon has been recorded with the virus strains in Australia in 2001; in France in 2000 and 2002; in Canada in 1999, 2000, 2001, and 2002; in Israel in 2002; and in the Netherlands in 2001 all being very closely related based on their F gene sequences.
[4] Overall, while vaccines and antiviral therapy treatments are in the works, the biggest difficulty that researchers face as of 2006[update] is the limited data available about the development of hMPV in the natural host.
[47] HMPV has been shown to circulate during fall and winter months with alternating predominance of a single subtype each year.
[49] American pharmaceutical corporation Moderna conducted a clinical trial for a candidate modRNA vaccine against metapneumovirus.
[53] The Chinese Center for Disease Control and Prevention published data showing that respiratory infections had risen significantly in the week of 16 to 22 December 2024;[54] human metapneumovirus was linked to 6.2 percent of positive respiratory illness tests and 5.4 percent of respiratory-illness hospitalizations in China, more than COVID-19, rhinovirus, or adenovirus.