Inguinal hernia
Symptoms, which may include pain or discomfort especially with or following coughing, exercise, or bowel movements, are absent in about a third of patients.
The inability to "reduce", or place the bulge back into the abdomen usually means the hernia is 'incarcerated' which requires emergency surgery.
In males, indirect hernias follow the same route as the descending testes, which migrate from the abdomen into the scrotum during the development of the urinary and reproductive organs.
[13] Inguinal hernias mostly contain the omentum or a part of the small intestines, however, some unusual contents may be an appendicitis, diverticulitis, colon cancer, urinary bladder, ovaries, and rarely malignant lesions.
[14] There are two types of inguinal hernia, direct and indirect, which are defined by their relationship to the inferior epigastric vessels.
As a result, the possibility for hernias through the inguinal canal in males is much greater because they have a larger opening and therefore a much weaker wall through which the intestines may protrude.
Since the abdominal walls weaken with age, direct hernias tend to occur in the middle-aged and elderly.
In the male fetus, the peritoneum gives a coat to the testicle as it passes through this ring, forming a temporary connection called the processus vaginalis.
The testicle remains connected to its blood vessels and the vas deferens, which make up the spermatic cord and descend through the inguinal canal to the scrotum.
When the opening is larger than necessary for passage of the spermatic cord, the stage is set for an indirect inguinal hernia.
The protrusion of peritoneum is not called "processus vaginalis" in women, as this structure is related to the migration of the testicle to the scrotum.
[citation needed] A physician may diagnose an inguinal hernia, as well as the type, from medical history and physical examination.
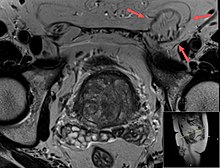
[20] For confirmation or in uncertain cases, medical ultrasonography is the first choice of imaging, because it can both detect the hernia and evaluate its changes with for example pressure, standing and Valsalva maneuver.
Large lipomas may appear nearly indistinguishable as the fat engulfs anatomic boundaries, but they do not change position with coughing or straining.
The more modern variety of truss is made with non-intrusive flat pads and comes with a guarantee to hold the hernia securely during all activities.
It is not recommended in minimally symptomatic hernias, for which watchful waiting is advised, due to the risk of post herniorraphy pain syndrome.
[28] Laparoscopy is most commonly used for non-emergency cases; however, a minimally invasive open repair may have a lower incidence of post-operative nausea and mesh associated pain.
During surgery conducted under local anaesthesia, the patient will be asked to cough and strain during the procedure to help in demonstrating that the repair is without tension and sound.
[29] Constipation after hernia repair results in strain to evacuate the bowel causing pain, and fear that the sutures may rupture.
[31] On the other hand, surgery has a risk of inguinodynia (10-12%), and this is why males with minimal symptoms are advised to watchful waiting.
[31][32] However, if they experience discomfort while doing physical activities or they routinely avoid them for fear of pain, they should seek surgical evaluation.








(photo: United States Military Medical Archives)
The photograph is blurry as the patient was shaking too much.