Steatosis
[3] Risk factors associated with steatosis are varied, and may include diabetes mellitus, protein malnutrition, hypertension,[4] cell toxins, obesity,[5] anoxia,[2] and sleep apnea.
No single mechanism leading to steatosis exists; rather, a varied multitude of pathologies disrupt normal lipid movement through the cell and cause accumulation.
Protein malnutrition, such as that seen in kwashiorkor, results in a lack of precursor apoproteins within the cell, therefore unused lipids which would normally participate in lipoprotein synthesis begin to accumulate.
[citation needed] Macrovesicular steatosis is the more common form of fatty degeneration and may be caused by oversupply of lipids due to obesity, obstructive sleep apnea (OSA),[8] insulin resistance, or alcoholism.
Nutrient malnutrition may also cause the mobilisation of fat from adipocytes and create a local oversupply in the liver where lipid metabolism occurs.
[citation needed] Microvesicular steatosis is characterized by small intracytoplasmic fat vacuoles (liposomes) which accumulate within hepatocytes.
[9] It is associated with a wide variety of conditions, including alcoholism, drug toxicity of several medications, delta hepatitis (in South America and Central Africa), sudden childhood death, congenital defects of fatty acid beta oxidation, cholesterol ester storage disease, Wolman disease and Alpers syndrome.
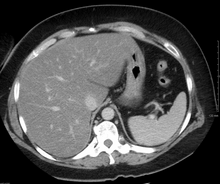
[citation needed] On X-ray computed tomography (CT), the increased fat component will decrease the density of the liver tissue, making the image less bright.
[citation needed] Several MRI vendors offer automated calculation of percent fat with acquisition sequences no longer than a single breath hold.