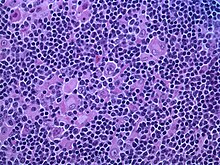
Nodular lymphocyte predominant Hodgkin lymphoma
[9] The LP cells have scant cytoplasm and one folded or multilobated nuclei with prominent, mostly basophilic nucleoli.
[10] Expert pathology review of multiple morphologic and immunophenotypic features[10] including the use of immunohistochemistry is essential.
[18] Surgical lymph node excision may be carried out at the time of diagnosis in certain cases such in children diagnosed at an early stage of progression.
[15] One study found sustained complete remission in half of the cases with a watch-and-wait strategy after surgical lymph node excision at the time of diagnosis.
[18][11] In one study, stage I-II patients treated with radiation therapy showed 10-year cause-specific survival of 98%, and the rate of developing radiotherapy-related second malignancies was not increased by the treatment (1% after 10 years).
[20] Recent management strategies recommend that Stage IA NLPHL without clinical risk factors should be treated with limited-field radiotherapy alone.
[18] Studies indicate Rituximab offers potential in relapsed or refractory patients,[22] and also in front-line treatment[4] especially in advanced stages.
[25] Prognosis is favourable in comparison with classic HL[20] despite a tendency for disease recurrence requiring long term followup.
[14] One study in the United States has suggested improved overall survival in response to chemotherapy for African Americans.