Otitis media
[2] One of the two main types is acute otitis media (AOM),[3] an infection of rapid onset that usually presents with ear pain.
[4][9] OME frequently occurs following AOM and may be related to viral upper respiratory infections, irritants such as smoke, or allergies.
[1] A number of measures decrease the risk of otitis media including pneumococcal and influenza vaccination, breastfeeding, and avoiding tobacco smoke.
[1] In children with otitis media with effusion antibiotics may increase resolution of symptoms, but may cause diarrhoea, vomiting and skin rash.
Since an episode of otitis media is usually precipitated by an upper respiratory tract infection (URTI), there are often accompanying symptoms like a cough and nasal discharge.
Trauma, such as a basilar skull fracture, can also lead to cerebrospinal fluid otorrhea (discharge of CSF from the ear) due to cerebral spinal drainage from the brain and its covering (meninges).
[18] This is usually due to inflammation of the mucous membranes in the nasopharynx, which can be caused by a viral upper respiratory tract infection (URTI), strep throat, or possibly by allergies.
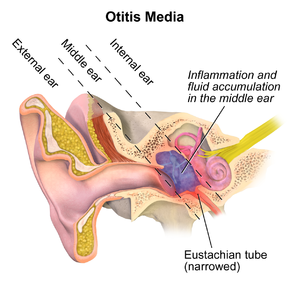
[19] By reflux or aspiration of unwanted secretions from the nasopharynx into the normally sterile middle-ear space, the fluid may then become infected – usually with bacteria.
In more severe cases, such as those with associated hearing loss or high fever, audiometry, tympanogram, temporal bone CT and MRI can be used to assess for associated complications, such as mastoid effusion, subperiosteal abscess formation, bony destruction, venous thrombosis or meningitis.
[23] Viral otitis may result in blisters on the external side of the tympanic membrane, which is called bullous myringitis (myringa being Latin for "eardrum").
If wax in the ear canal obscures a clear view of the eardrum it should be removed using a blunt cerumen curette or a wire loop.
An upset young child's crying can cause the eardrum to look inflamed due to distension of the small blood vessels on it, mimicking the redness associated with otitis media.
[25] The most common bacteria isolated from the middle ear in AOM are Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis,[1] and Staphylococcus aureus.
[28] An effusion can cause conductive hearing loss if it interferes with the transmission of vibrations of middle ear bones to the vestibulocochlear nerve complex that are created by sound waves.
Prolonged inflammation leads to middle ear swelling, ulceration, perforation, and attempts at repair with granulation tissue and polyps.
Risk factors include poor eustachian tube function, recurrent ear infections, crowded living, daycare attendance, and certain craniofacial malformations.
[32] Pneumococcal conjugate vaccines (PCV) in early infancy decrease the risk of acute otitis media in healthy infants.
[33] Risk factors such as season, allergy predisposition and presence of older siblings are known to be determinants of recurrent otitis media and persistent middle-ear effusions (MEE).
A 2023 review found evidence for the effectiveness of single or combinations of oral pain relief in acute otitis media is limited.
For people requiring surgery to treat otitis media with effusion, preventative antibiotics may not help reduce the risk of post-surgical complications.
[50] For bilateral acute otitis media in infants younger than 24 months, there is evidence that the benefits of antibiotics outweigh the harms.
[12] A 2015 Cochrane review concluded that watchful waiting is the preferred approach for children over six months with non severe acute otitis media.
[58] The decision to treat is usually made after a combination of physical exam and laboratory diagnosis, with additional testing including audiometry, tympanogram, temporal bone CT and MRI.
[64][65] In more severe cases, tympanostomy tubes can be inserted,[57] possibly with adjuvant adenoidectomy[59] as it shows a significant benefit as far as the resolution of middle ear effusion in children with OME is concerned.
[14] In severe or untreated cases, the tympanic membrane may perforate, allowing the pus in the middle-ear space to drain into the ear canal.
In a simple case of acute otitis media in an otherwise healthy person, the body's defenses are likely to resolve the infection and the ear drum nearly always heals.
Prolonged duration of otitis media is associated with ossicular complications and, together with persistent tympanic membrane perforation, contributes to the severity of the disease and hearing loss.
When a cholesteatoma or granulation tissue is present in the middle ear, the degree of hearing loss and ossicular destruction is even greater.
[80] Once the infections resolve and hearing thresholds return to normal, childhood otitis media may still cause minor and irreversible damage to the middle ear and cochlea.
[83] Andrew Butcher speculates that the lack of fricatives and the unusual segmental inventories of Australian languages may be due to the very high presence of otitis media ear infections and resulting hearing loss in their populations.


|
no data
< 10
10–14
14–18
18–22
22–26
26–30
|
30–34
34–38
38–42
42–46
46–50
> 50
|
