Tetraplegia
Tetraplegia, also known as quadriplegia, is defined as the dysfunction or loss of motor and/or sensory function in the cervical area of the spinal cord.
(Paraplegia is similar but affects the thoracic, lumbar, and sacral segments of the spinal cord and arm function is retained.
[2] A loss of sensory function can present as an impairment or complete inability to sense light touch, pressure, heat, pinprick/pain, and proprioception.
[3] Secondarily, because of their depressed functioning and immobility, tetraplegics are often more vulnerable to pressure sores, osteoporosis and fractures, frozen joints, spasticity, respiratory complications, infections, autonomic dysreflexia, deep vein thrombosis, and cardiovascular disease.
An individual with an injury at C1 (the highest cervical vertebra, at the base of the skull) will probably lose function from the neck down and be ventilator-dependent.
An individual in between, with a C5 injury may lose some function from the chest down and fine motor skills in his/her hands but still have flexion and extension abilities of certain muscles around the back or arm area.
A partial severing or even bruising of the spinal cord results in varying degrees of mixed function and paralysis.
A common misconception with tetraplegia is that the victim cannot move legs, arms, or any other major body regions; this is often not the case.
[3] It is common to have partial movement in limbs, such as the ability to move the arms but not the hands, or to be able to use the fingers but not to the same extent as before the injury.
The injury, which is known as a lesion, causes the loss of partial or total function of all four limbs, meaning the arms and the legs.
Typical causes of this damage are trauma (such as a traffic collision, diving into shallow water, a fall, a sports injury), disease (such as transverse myelitis, Guillain–Barré syndrome, multiple sclerosis, or polio), or congenital disorders (such as muscular dystrophy).
[6] Parkinson's disease Tetraplegia is defined in many ways; C1–C4 usually affects arm movement more so than a C5–C7 injury; however, all tetraplegics have or have had some kind of finger dysfunction.
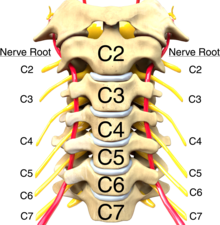
To understand how tetraplegia presents after injury, it is imperative to have a broad knowledge of the cervical spinal roots and its many functions.
This is typically done at 72 hours post-injury; exams done prior to this time have been found to be inaccurate due to the presence of swelling and other confounding factors.
[9] Patients with an incomplete lesion also often need therapy or surgery before the procedure to restore function to correct the consequences of the injury.
When upper limb function is absent as a result of a spinal cord injury it is a major barrier to regain autonomy.
Individuals with C5 injuries retain some function in their biceps, deltoids, and other muscles; they typically can perform many ADLs including feeding, bathing, and grooming but require total assistance with bowel/bladder care.
The C6 level adds function in the extensor carpi radialis, longus, and other muscles allowing for wrist extension, scapular abduction, and wrist flexion; typically, these patients have modified independent feeding and grooming with adaptive equipment, independent with dressing, can use both a manual and power wheelchair but require assistance with some activities of daily living.
[11] In the case of cerebral palsy, which is caused by damage to the motor cortex either before, during (10%), or after birth, some people with incomplete tetraplegia are gradually able to learn to stand or walk through physical therapy.
Combining resistance training with proper nutrition intake can greatly reduce co-morbidities such as obesity and type 2 diabetes.
Medical literature favors using "tetraplegia" as the standardized term, as it is frowned upon to mix Greek and Latin roots, although "quadriplegia" remains in use.