Rhinitis
[6] Allergic rhinitis may cause additional symptoms, such as sneezing and nasal itching, coughing, headache,[7] fatigue, malaise, and cognitive impairment.
When mast cells degranulate, they release histamine and other chemicals,[10] starting an inflammatory process that can cause symptoms outside the nose, such as fatigue and malaise.
Symptoms of the common cold include rhinorrhea, sneezing, sore throat (pharyngitis), cough, congestion, and slight headache.
The category was formerly referred to as vasomotor rhinitis, as the first cause discovered was vasodilation due to an overactive parasympathetic nerve response.
[23] There is still much to be learned about this, but it is thought that these non-allergic triggers cause dilation of the blood vessels in the lining of the nose, which results in swelling and drainage.
Overexpression of these receptors have influence the nasal airway hyper-responsiveness to non-allergic irritant environmental stimuli (e.g., extremes of temperature, changes in osmotic or barometric pressure).
[26] Vasomotor rhinitis appears to be significantly more common in women than men, leading some researchers to believe that hormone imbalance plays a role.
[29] In other populations, particularly those of European descent, a genetic variant in the gene that metabolizes ethanol to acetaldehyde, ADH1B, is associated with alcohol-induced rhinitis.
[31] Aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs), particularly those that inhibit cyclooxygenase 1 (COX1), can worsen rhinitis and asthma symptoms in individuals with a history of either one of these diseases.
A systematic review on non-allergic rhinitis reports improvement of overall function after treatment with capsaicin (the active component of chili peppers).
[35] Allergic rhinitis or hay fever may follow when an allergen such as pollen, dust, or Balsam of Peru[36] is inhaled by an individual with a sensitized immune system, triggering antibody production.
Rhinitis medicamentosa is a form of drug-induced nonallergic rhinitis which is associated with nasal congestion brought on by the use of certain oral medications (primarily sympathomimetic amine and 2-imidazoline derivatives) and topical decongestants (e.g., oxymetazoline, phenylephrine, xylometazoline, and naphazoline nasal sprays) that constrict the blood vessels in the lining of the nose.
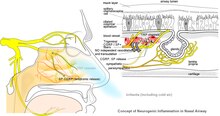
[41] Neurogenic inflammation produced by neuropeptides released from sensory nerve endings to the airways is a proposed common mechanism of association between both allergic and non-allergic rhinitis with asthma.
Among the causative agents are flours, enzymes used in processing food, latex, isocyanates, welding fumes, epoxy resins, and formaldehyde.
[clarification needed] Vasomotor rhinitis is differentiated from viral and bacterial infections by the lack of purulent exudate and crusting.
[44] Evidence has been published from a few health apps for mobile devices that show potential to assist in the diagnosis of rhinitis and rhinosinusitis and to evaluate management and treatment adherence.
While this shows promise for clinical management, as of 2022[update] few had been validated in the scientific literature, and even fewer included considerations for multimorbidity.