1826–1837 cholera pandemic
[3][4] The medical community now believes cholera to be exclusively a human disease, spread through many means of travel during the time, and transmitted through warm fecal-contaminated river waters and contaminated foods.
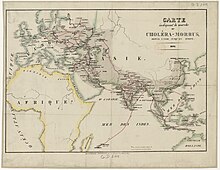
The first cholera pandemic (1817–24) began near Kolkata and spread throughout Southeast Asia to the Middle East, eastern Africa, and the Mediterranean coast.
While cholera had spread across India many times previously, this outbreak went farther; it reached as far as China and the Mediterranean Sea before receding.
Hundreds of thousands of people died as a result of this pandemic, including many British soldiers, which attracted European attention.
[17] By late summer, with the disease appearing more likely to spread to Britain, its board of health, in accordance with the prevailing miasma theory, issued orders recommending as a preventive the burning of "decayed articles, such as rags, cordage, papers, old clothes, hangings...filth of every description removed, clothing and furniture should be submitted to copious effusions of water, and boiled in a strong ley (lye); drains and privies thoroughly cleansed by streams of water and chloride of lime...free and continued admission of fresh air to all parts of the house and furniture should be enjoined for at least a week".
[18] Based on the reports of two English doctors who had observed the epidemic in Saint Petersburg, the board of health published a detailed description of the disease's symptoms and onset: Giddiness, sick stomach, nervous agitation, intermittent, slow, or small pulse, cramps beginning at the tops of the fingers and toes, and rapidly approaching the trunk, give the first warning.
Vomiting or purging, or both these evacuations of a liquid like rice-water or whey, or barley-water, come on; the features become sharp and contracted, the eye sinks, the look is expressive of terror and wildness; the lips, face, neck, hands, and feet, and soon after the thighs, arms, and whole surface assume a leaden, blue, purple, black, or deep brown tint according to the complexion of the individual, varying in shade with the intensity of the attack.
The nails put on a bluish pearly white; the larger superficial veins are marked by flat lines of a deeper black; the pulse becomes either small as a thread, and scarcely vibrating, or else totally extinct.
The secretion of urine is totally suspended; vomiting and purgings, which are far from being the most important or dangerous symptoms, and which in a very great number of cases of the disease, have not been profuse, or have been arrested by medicine early in the attack, succeed.
It is evident that the most urgent and peculiar symptom of this disease is the sudden depression of the vital powers: proved by the diminished action of the heart, the coldness of the surface and extremities, and the stagnant state of the whole circulation.
[19]From September 1831 to January 1832, a catastrophic cholera epidemic ravaged the lower Euphrates and Tigris regions of what is now Iraq and Iran.
The United States believed that cholera was brought by recent immigrants, specifically the Irish, and epidemiologists understand they were carrying disease from British ports.
[25][26][27] In response to the second cholera pandemic, the Ottoman Empire and Egypt reformed their quarantine systems, following the western Mediterranean model.
Latta established from blood studies that a saline drip greatly improved the condition of patients and saved many lives by preventing dehydration.