Alpha-1 blocker
They are mainly used to treat benign prostatic hyperplasia (BPH), hypertension and post-traumatic stress disorder.
[3][5] Tamsulosin is not centrally active due to poor blood-brain barrier penetration, but terazosin and prazosin are centrally-active.
[1][2][7][8] Doxazosin, terazosin, alfuzosin, and tamsulosin have all been well established in treatment to reduce lower urine tract symptoms (LUTS) caused by benign prostatic hyperplasia.
First generation alpha-1 blockers, like prazosin are not recommended to treat lower urinary tract symptoms because of their blood-pressure-lowering effect.
Dutasteride and tamsulosin are on the market as combined therapy and results have shown that they improve symptoms significantly versus monotherapy.
This is supported by studies that show surprisingly though consistently that neither alpha- nor beta-blocker mono- therapy reduces sympathetically mediated blood pressure reactivity to acute experimental stressors.
In these studies, doxazosin was prescribed at the low dose of 1–2 mg. [16] [17] [18] Post-traumatic stress disorder (PTSD) is a disabling mental condition that can develop following a traumatic experience; for example, it is especially common in military veterans and sexual assault survivors.
Prazosin is commonly used as an antihypertensive, but because alpha-1-adrenergic activity has been connected to fear and startle responses, it sees use as a PTSD treatment.
The risk of first dose phenomenon may be reduced or eliminated by gradual-dose titration, since the adverse effects of Prazosin are dose-related.
Contraindication : Allergies or hypersensitivity to alpha-1 blockers or any of the active ingredient, that includes angiodema induced by the drug.
[32][33] Since alpha-1 blockers may cause orthostatic hypotension, co-administration with antihypertensives and vasodilators must be evaluated with regards to risk-benefit as the risk for low blood pressure is greatly increased.
As discussed above, tamsulosin may have less risk for low blood pressure and orthostatic hypotension due to its selectivity for α1a-adrenergic receptors.
Silodosin shows high affinity and selectivity for alpha-1a adrenergic receptors found in the prostate which ensures that it works quickly and effectively to relieve the symptoms of BPH.
Distribution volume and excretion increases with renal impairment due to less protein binding, but the half-life elimination rate is unchanged.
Delay in elimination half-life, peak concentration in plasma is double and bioavailability is changed in hepatic impairment patients.
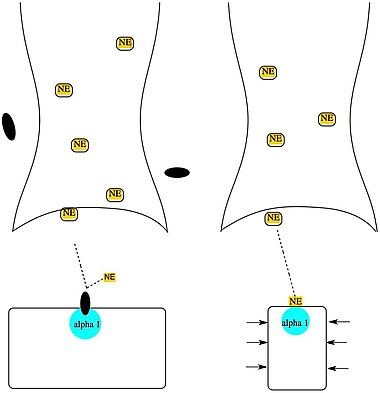
[39][42] Alpha-1 blockers inhibit the activation of post-synaptic alpha-1 receptors by norepinephrine thus opposing blood vessel contraction.
It helps the urine to flow smoothly and it can lessen the pain caused by the bladder pressing on the prostate.
[2] Terazosin, tamsulosin and doxazosin are prime drug for BPH because they have a long half-life and modified release formulation.
[46][47] Alpha-1 blockers have a good effect on lipoproteins in plasma, insulin resistance and it causes the glucose levels in blood to lower.
[52] The first effective treatment for benign prostatic hyperplasia (BPH) was a non-selective alpha blocker phenoxybenzamine which was irreversible.
Prazosin was synthesized in 1974 when Constantin and Hess were trying to discover a vasodilator which had a minimal effect on cardiac activity.
[7] Prazosin was a much better tolerated drug than phenoxybenzamine but the problem still remained that it lowered the blood pressure more than desired for a BPH treatment.
Alfuzosin SR (sustained release) was the fourth alpha 1 selective blocker to be approved by FDA and requires no dose titration.