Calprotectin
[9] Calprotectin comprises as much as 60% of the soluble protein content of the cytosol of a neutrophil,[2][10][11] and it is secreted by an unknown mechanism during inflammation.
[3] Faecal calprotectin has been used to detect intestinal inflammation (colitis or enteritis) and can serve as a biomarker for inflammatory bowel diseases.
[16] Early size exclusion chromatography experiments incorrectly indicated that calprotectin had a molecular mass of 36.5 kDa;[2][11] occasionally this value is used in contemporary literature.
[18] Calcium binding induces a conformational change in the complex that improves its affinity for transition metals, and promotes tetramer formation.
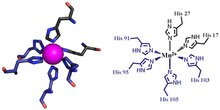
[9] In hexa-histidine binding two further histidine residues, His103 and His105, are recruited from the C-terminal end of S100A9 to enable octahedral coordination of the transition metal.
[9][19] Calprotectin constitutes up to 60% of soluble protein content in the cytosol of neutrophil granulocytes,[2][10][11] and it can be found at a lower concentration in monocytes, macrophages, and squamous epithelial cells.
Circulating activated platelets and platelet-leukocyte aggregates are increased in acute and chronic sterile thrombo-inflammatory diseases.
[3] In lung autopsies from patients with inflammation caused by COVID-19, heterodimeric S100A8/A9 is mainly detected in neutrophils and deposited on vessel walls.
The prothrombotic pathway initiated by interaction of S100A8/A9 with GPIbα induces the formation of procoagulant platelets and fibrin (CD36 has a supporting role).
[24] Mammals strictly limit metal availability as a part of the innate immune system, and this helps prevent infection by microbes and fungi.
[27] Furthermore, positive faecal calprotectin does not help in localizing IBD, or in distinguishing ulcerative colitis from Crohn's disease.
[1] Faecal calprotectin could be used as a preliminary screen in otherwise functional patients suspected of having IBD, or as a means of following mucosal healing.