Comparison of the healthcare systems in Canada and the United States
Some 59% of U.S. residents have access to health care insurance through employers, although this figure is decreasing, and coverages as well as workers' expected contributions vary widely.
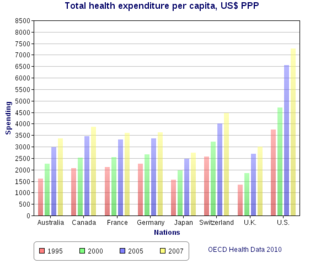
[23] Despite the greater role of private business in the US, federal and state agencies are increasingly involved, paying about 45% of the $2.2 trillion the nation spent on medical care in 2004.
[26] The Canadian system has been 69–75% publicly funded,[27] though most services are delivered by private providers, including physicians (although they may derive their revenue primarily from government billings).
In Canada, emergency room treatment for legal Canadian residents is not charged to the patient at time of service but is met by the government.
The same survey states that 37% of Canadians say it is difficult to access care after hours (evenings, weekends or holidays) without going to the emergency department compared to over 34% of Americans.
[55] A 2018 survey conducted by the Fraser Institute, a conservative-libertarian public policy think tank, found that wait times in Canada for a variety of medical procedures reached "an all-time high".
[57] In response to these findings, the Physicians for a National Health Program (PNHP), an advocacy organization comprising more than 20,000 American medical professionals, identified statistical problems with the Fraser Institute's reporting.
Conversely, a study conducted by the Canadian Institute for Health Information indicated that Canada has been successful in delivering care within medically recommended wait times.
In July 2009 Holmes agreed to appear in television ads broadcast in the United States warning Americans of the dangers of adopting a Canadian-style health care system.
After her ad appeared critics pointed out discrepancies in her story, including that Rathke's cleft cyst, the condition she was treated for, was not a form of cancer, and was not life-threatening.
The report concluded by observing that gap between U.S. and Canadian spending on administration had grown to $752 per capita and that a large sum might be saved in the United States if the U.S. implemented a Canadian-style system.
[81] Illegal immigrants, more prevalent in the U.S. than in Canada,[citation needed] also add a burden to the system, as many of them do not carry health insurance and rely on emergency rooms — which are legally required to treat them under EMTALA — as a principal source of care.
However, statistics published in 2005 by the Canadian Institute for Health Information (CIHI), show that, for the first time since 1969 (the period for which data are available), more physicians returned to Canada than moved abroad.
[12] In 2007, Gordon H. Guyatt et al. conducted a meta-analysis, or systematic review, of all studies that compared health outcomes for similar conditions in Canada and the U.S., in Open Medicine, an open-access peer-reviewed Canadian medical journal.
They concluded, "Available studies suggest that health outcomes may be superior in patients cared for in Canada versus the United States, but differences are not consistent."
Guyatt identified 38 studies addressing conditions including cancer, coronary artery disease, chronic medical illnesses and surgical procedures.
The U.S. performed better on 6 indicators, including survival rates for breast and cervical cancer, and avoidance of childhood diseases such as pertussis and measles.
[133] A 2004 study found that Canada had a slightly higher mortality rate for acute myocardial infarction (heart attack) because of the more conservative Canadian approach to revascularizing (opening) coronary arteries.
[135] Dr. Barry Kramer of the National Institutes of Health points to the fact that cancer incidence rose sharply over the past few decades as screening became more common.
Incidence rates for certain types, such as colorectal and stomach cancer, were actually higher in Canada than in the U.S.[139] In 2004, researchers published a study comparing health outcomes in the Anglo countries.
[143] Echoing the concerns of Dr. Kramer and Professor Mackillop, Hsing later wrote that reported prostate cancer incidence depends on screening.
[citation needed] Since 1998, Canada's successive multibillion-dollar budget surpluses have allowed a significant injection of new funding to the healthcare system, with the stated goal of reducing waiting times for treatment.
[citation needed] In the U.S., President Bill Clinton attempted a significant restructuring of health care, but the effort collapsed under political pressure against it despite tremendous public support.
[160] In 2006, Massachusetts adopted a plan that vastly reduced the number of uninsured making it the state with the lowest percentage of non-insured residents in the union.
[161] In 2009, in a minor amendment, the plan did eliminate dental, hospice and skilled nursing care for certain categories of noncitizens covering 30,000 people (victims of human trafficking and domestic violence, applicants for asylum and refugees) who do pay taxes.
[162][163] In July 2009, Connecticut passed into law a plan called SustiNet, with the goal of achieving health care coverage of 98% of its residents by 2014.
[167] Governments attempt to control health care costs by being the sole purchasers and thus they do not allow private patients to bid up prices.
[169][170] In the United States, Congress has enacted laws to promote consumer-driven healthcare with health savings accounts (HSAs), which were created by the Medicare bill signed by President George W. Bush on December 8, 2003.
HSAs are designed to provide tax incentives for individuals to save for future qualified medical and retiree health expenses.
This concern was one of the driving factors behind a provision of the Patient Protection and Affordable Care Act, informally known as Obamacare, which limited the types of purchases which could be made with HSA funds.