Colitis-X
Hypovolemic and endotoxic shock are manifest by increased capillary refill time, congested or cyanotic (purplish) mucous membranes, and cold extremities.
[1][2] Clinical signs are similar to those of other diarrheal diseases, including toxemia caused by Clostridium, Potomac horse fever, experimental endotoxic shock, and anaphylaxis.
[1] To date, the precise causative factor has not been verified, and the disease has been attributed by various sources to viruses, parasites, bacteria, use of antibiotics and sulfonamides, and heavy metal poisoning.
[7] The link to stress suggests the condition may be brought on by changes in the microflora of the cecum and colon that lower the number of anaerobic bacteria, increase the number of Gram-negative enteric bacteria, and decrease anaerobic fermentation of soluble carbohydrates, resulting in damage to the cecal and colonic mucosa and allowing increased absorption of endotoxins from the lumen of the gut.
In a 2009 study at the University of Arizona, C. difficile toxins A and B were detected, large numbers of C. difficile were isolated, and genetic characterization revealed them to be North American pulsed-field gel electrophoresis type 1, polymerase chain reaction ribotype 027, and toxinotype III.
The individual animal studied in this case was diagnosed as having peracute typhlocolitis, with lesions and history typical of those attributed to colitis X.
[11] In humans, C. difficile is the most serious cause of antibiotic-associated diarrhea, often a result of eradication of the normal gut flora by antibiotics.
[11] At necropsy, edema and hemorrhage in the wall of the large colon and cecum are pronounced, and the intestinal contents are fluid and often blood-stained.
[1] Macroscopic and microscopic findings include signs of disseminated intravascular coagulation, necrosis of colonic mucosa and presence of large numbers of bacteria in the devitalized parts of the intestine.
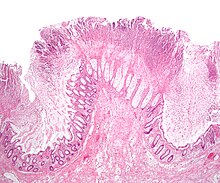
Histopathologically, the mucosa of the large colon is hemorrhagic, necrotic, and covered with fibrohemorrhagic exudate, while the submucosa, the muscular tunic, and the local lymph nodes are edematous.
[1] Mortality rate has been theorized to fall to 75% if treatment is prompt and aggressive, including administration of not only fluids and electrolytes, but also blood plasma, anti-inflammatory and analgesic drugs, and antibiotics.