Slow-wave sleep
[3] SWS is characterised by moderate muscle tone, slow or absent eye movement, and lack of genital activity.
The second section of the wave signifies an "up state", an excitation or depolarizing phase in which the neurons fire briefly at a high rate.
A central model has been hypothesized that long-term memory storage is facilitated by an interaction between the hippocampal and neocortical networks.
[15] In addition, a correlation can be observed between the amplitude of hippocampal activity during SWS and the improvement in spatial memory performance, such as route retrieval, on the following day.
[15] A separate study found that when subjects hear sounds associated with previously shown pictures of locations, the reactivation of individual memory representations was significantly higher during SWS as compared to other sleep stages.
Emotions with negative salience presented as a cue during SWS show better reactivation, and therefore an enhanced consolidation in comparison to neutral memories.
Considering that acetylcholine is a neurotransmitter that modulates the direction of information flow between the hippocampus and neocortex during sleep, its suppression is necessary during SWS to consolidate sleep-related declarative memory.
Stage N3 is defined by the presence of 20% delta waves in any given 30-second epoch of the EEG during sleep, by the current 2007 AASM guidelines.
[7][20] Longer periods of SWS occur in the first part of the night, primarily in the first two sleep cycles (roughly three hours).
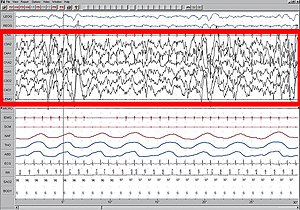
[citation needed] NREM sleep, as observed on the electroencephalogram (EEG), is distinguished by certain characteristic features.
Indeed, a study reported a unilateral activation of the somatosensorial cortex when a vibrating stimulus was put on the hand of human subjects.
SWS is therefore sensitive to danger and a non-familiar environment, creating a need for vigilance and reactivity during sleep.
[27] Several neurotransmitters are involved in sleep and waking patterns: acetylcholine, norepinephrine, serotonin, histamine, and orexin.
Also, these neurons appear to have some form of internal dialogue, which accounts for the mental activity during this state where there is no information from external signals (because of the synaptic inhibition at the thalamic level).
Growth hormone is also secreted during this stage, which leads some scientists to hypothesize that a function of slow-wave sleep is to facilitate the healing of muscles as well as repair damage to tissues.
An individual will sleep-walk leaving his or her bed in the middle of the night seeking out food, and will eat not having any memory of the event in the morning.
A. Horne (1978) reviewed several experiments with humans and concluded that sleep deprivation has no effects on people's physiological stress response or ability to perform physical exercise.
The regions of the brain that are most active when awake have the highest level of delta waves during slow-wave sleep.
The "shutting down" of the brain accounts for the grogginess and confusion if someone is awakened during deep sleep since it takes the cerebral cortex time to resume its normal functions.
In slow-wave sleep, the decreased rate of metabolism reduces the creation of oxygen byproducts, thereby allowing the existing radical species to clear.
[34] A good candidate for slow wave activity (SWA), which occurs during deep non-REM sleep, is amyloid-b modulation.
These structural anomalies are linked to disruptions in the sleep-wake cycle, particularly in non-rapid eye movement (NREM), slow wave sleep (SWS).
The results showed that there was a lower percentage of SWS in African Americans compared to Caucasians, but since there are many influencing factors (e.g., body mass index, sleep-disordered breathing, obesity, diabetes, and hypertension), this potential difference must be investigated further.
[39] Mental disorders play a role in individual differences in the quality and quantity of SWS: subjects with depression show a lower amplitude of slow-wave activity (SWA) compared to healthy participants.
Sex differences also persist in the former group: depressed men present significantly lower SWA amplitude.
[41] During sleep, the distribution of slow-wave activity (SWA) typically exhibits a prevalence in the frontal region of the brain.
The administration of the GABAa agonist gabaxadol enhances both deep sleep and also positively impacts various indicators of insomnia.
[52] Tiagabine, a selective gamma-aminobutyric acid (GABA) reuptake inhibitor, demonstrated to shown to improve sleep maintenance and to significantly increase SWS in healthy elderly subjects and adult patients with primary insomnia.
[57][58] Levodopa is a drug commonly used to treat Parkinson's disease which acts to increases the brain's dopamine availability.