Hepatitis
[3][5] Some people or animals with hepatitis have no symptoms, whereas others develop yellow discoloration of the skin and whites of the eyes (jaundice), poor appetite, vomiting, tiredness, abdominal pain, and diarrhea.
[22][23] Cases of drug-induced hepatitis can manifest with systemic signs of an allergic reaction including rash, fever, serositis (inflammation of membranes lining certain organs), elevated eosinophils (a type of white blood cell), and suppression of bone marrow activity.
[19][20] As the inflammation progresses, patients can develop constitutional symptoms similar to acute hepatitis, including fatigue, nausea, vomiting, poor appetite, and joint pain.
[20] Chronic hepatitis interferes with hormonal functions of the liver which can result in acne, hirsutism (abnormal hair growth), and amenorrhea (lack of menstrual period) in women.
[41] The National Institutes of Health maintains the LiverTox Archived 2019-07-24 at the Wayback Machine database for consumers to track all known prescription and non-prescription compounds associated with liver injury.
[44] Non-alcoholic liver disease occurs in people with little or no history of alcohol use, and is instead strongly associated with metabolic syndrome, obesity, insulin resistance and diabetes, and hypertriglyceridemia.
[17] The chronic presence of the virus within liver cells results in multiple waves of inflammation, injury and wound healing that over time lead to scarring or fibrosis and culminate in hepatocellular carcinoma.
[17] Natural killer cells are the primary drivers of the initial innate response and create a cytokine environment that results in the recruitment of CD4 T-helper and CD8 cytotoxic T-cells.
[65][66][67] This initially reversible process overwhelms the hepatocyte's ability to maintain lipid homeostasis leading to a toxic effect as fat molecules accumulate and are broken down in the setting of an oxidative stress response.
[65][66][67] Over time, this abnormal lipid deposition triggers the immune system via toll-like receptor 4 (TLR4) resulting in the production of inflammatory cytokines such as TNF that cause liver cell injury and death.
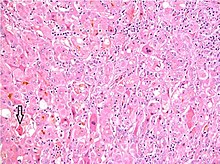
[33] In this case, liver biopsy is the gold standard for establishing the diagnosis: histopathologic analysis is able to reveal the precise extent and pattern of inflammation and fibrosis.
[33] Biopsy is typically not the initial diagnostic test because it is invasive and is associated with a small but significant risk of bleeding that is increased in people with liver injury and cirrhosis.
[77] Liver biopsies show identical findings in patients with ASH and NASH, specifically, the presence of polymorphonuclear infiltration, hepatocyte necrosis and apoptosis in the form of ballooning degeneration, Mallory bodies, and fibrosis around veins and sinuses.
If HBsAg is present, a second test – usually done on the same blood sample – that detects the antibody for the hepatitis B core antigen (anti-HBcAg) can differentiate between acute and chronic infection.
[99] Because hepatitis A is transmitted primarily through the oral-fecal route, the mainstay of prevention aside from vaccination is good hygiene, access to clean water and proper handling of sewage.
As there is a dearth of clinical trial data and the drugs used to treat are prone to developing resistance, experts recommend reserving treatment for severe acute cases, not mild to moderate.
[20] Seven drugs are approved in the United States:[20] First-line treatments currently used include PEG IFN, entecavir, and tenofovir, subject to patient and physician preference.
[112][113] The indirect acting antivirals include pegylated interferon (PEG IFN) and ribavirin (RBV), which in combination have historically been the basis of therapy for HCV.
[17] Specific populations at greatest risk include: travelers to endemic regions, men who have sex with men, those with occupational exposure to non-human primates, people with clotting disorders who have received clotting factors, people with history of chronic liver disease in whom co-infection with hepatitis A can lead to fulminant hepatitis, and intravenous drug users (rare).
[17][106] A history of intravenous drug injection is the most important risk factor for chronic hepatitis C.[132] Other susceptible populations include those engaged in high-risk sexual behavior, infants of infected mothers, and healthcare workers.
Henry Beecher was one of the foremost critics in an article in the New England Journal of Medicine in 1966, arguing that parents were unaware to the risks of consent and that the research was done to benefit others at the expense of children.
[147] Moreover, he argued that poor families with mentally disabled children often felt pressured to join the research project to gain admission to the school, with all of the educational and support resources that would come along with it.
He travelled across the globe collecting blood samples, investigating the interplay between disease, environment, and genetics with the goal of designing targeted interventions for at-risk people that could prevent them from getting sick.
Blumberg continued to study the antigen, and eventually developed the first hepatitis B vaccine using plasma rich in HBsAg, for which he received the Nobel Prize in Medicine in 1976.
[163] The largest outbreak of hepatitis A virus in United States history occurred among people who ate at a now-defunct Mexican food restaurant located in Monaca, Pennsylvania in late 2003.
[164] The outbreak was brought to the attention of health officials when local emergency medicine physicians noticed a significant increase in cases of hepatitis A in the county.
[164] The CDC believes that the restaurant's use of a large communal bucket for chopped raw green onion allowed non-contaminated plants to be mixed with contaminated ones, increasing the number of vectors of infection and amplifying the outbreak.
[88][168] Based on the limited available evidence, the American Association for the Study of Liver Diseases (AASLD) recommends antiviral therapy in pregnant women whose viral load exceeds 200,000 IU/mL.
[171][172] A 2010 systematic review and meta-analysis found that Lamivudine initiated early in the third trimester also significantly reduced mother-to-child transmission of HBV, without any known adverse effects.
[88][90] Pregnant women who contract HEV are at significant risk of developing fulminant hepatitis with maternal mortality rates as high as 20–30%, most commonly in the third trimester .