Vertebral augmentation
These medical terms are classical compounds of the suffix -plasty meaning "molding or shaping surgically" (from Ancient Greek plastós "molded, formed") and the prefixes vertebro- "vertebra" (from Latin vertebra "joint, joint of the spine") and kypho- "humped; stooping forward" (from Ancient Greek kyphos "crooked").
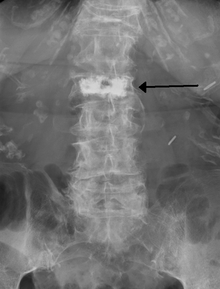
[2] Kyphoplasty is a variation of a vertebroplasty which attempts to restore the height and angle of kyphosis of a fractured vertebra (of certain types), followed by its stabilization using injected bone cement.
The procedure typically includes the use of a small balloon that is inflated in the vertebral body to create a void within the cancellous bone prior to cement delivery.
[7] The subjects in these trials had primarily non-acute fractures and prior to the release of the results they were considered the most ideal people to receive the procedure.
[8][9] A number of non-blinded trials suggested effectiveness,[10] but the lack of blinding limits what can be concluded from the results and some have been criticized because of being funded by the manufacturer.
[13] Others consider the procedure only appropriate for those with other health problems making rest possibly detrimental, those with metastatic cancer as the cause of the spine fracture, or those who do not improve with conservative management.
[14] Evidence does not support a benefit of kyphoplasty over vertebroplasty with respect to pain, but the procedures may differ in restoring lost vertebral height, and in safety issues like cement extravasation (leakage).
[18][19][20] In 2010, the board of directors of the American Academy of Orthopaedic Surgeons released a statement recommending strongly against use of vertebroplasty for osteoporotic spinal compression fractures,[21] while the Australian Medical Services Advisory Committee considers both vertebroplasty and kyphoplasty only to be appropriate in those who have failed to improve after a trial of conservative treatment,[22] with conservative treatment (analgesics primarily) being effective in two-thirds of people.
Although severe complications are extremely rare, infection, bleeding, numbness, tingling, headache, and paralysis may ensue because of misplacement of the needle or cement.
The first percutaneous vertebroplasty was performed in 1984 at the University Hospital of Amiens, France to fill a vertebral void left after the removal of a benign spinal tumor.
NAS states that in order to be reimbursable, a procedure must meet certain criteria, including, 1) a detailed and extensively documented medical record showing pain caused by a fracture, 2) radiographic confirmation of a fracture, 3) that other treatment plans were attempted for a reasonable amount of time, 4) that the procedure is not performed in the emergency department, and 5) that at least one year of follow-up is planned for, among others.
[33] In 2015, it was reported by The Atlantic that a person associated with a medical device company that sells equipment related to the kyphoplasty procedure had edited the Wikipedia article on the subject to promote claims about its efficacy.