Selective androgen receptor modulator
Selective androgen receptor modulators (SARMs) are a class of drugs that selectively activate the androgen receptor in specific tissues, promoting muscle and bone growth while having less effect on male reproductive tissues like the prostate gland.
SARMs have been investigated in human studies for the treatment of osteoporosis, cachexia (wasting syndrome), benign prostatic hyperplasia, stress urinary incontinence, and breast cancer.
As of 2023[update], there are no SARMs which have been approved by the United States Food and Drug Administration or the European Medicines Agency.
SARMs are readily available on internet-based gray markets and are commonly used recreationally to stimulate muscle growth.
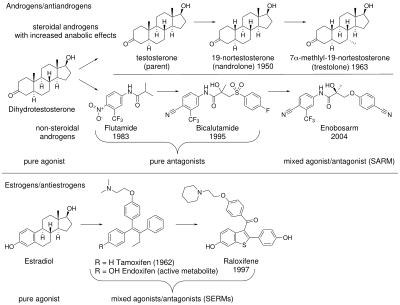
AAS effects can be separated into androgenic (the development and maintenance of male sexual characteristics) and anabolic (increasing bone density, muscle mass and strength).
[6][7] For most medical applications, an AAS with potent anabolic and minimal androgenic and cardiovascular effects would be an advantage.
[12] Interest in nonsteroidal AR mixed agonists/antagonists increased after the therapeutic uses of selective estrogen receptor modulators (SERMs) became evident.
[16] The clinical success of SERMs stimulated interest in analogous tissue selective drugs that target the AR.
These antagonists work by binding to the AR to prevent androgenic action; this class of chemicals dates to the 1970s.
[6][13] The discovery of arylpropionamides, which share structural similarity with bicalutamide and hydroxyflutamide, suggested a way to make compounds that bind to the AR and produce both anabolic and antiandrogenic effects.
[17][18][19] Phase I and II trials have provided preliminary evidence that the SARMs enobosarm and GSK-2881078 (in elderly men and postmenopausal women), and OPL-88004 (prostate cancer survivors with low levels of testosterone) increase lean body mass and muscle size with little effect on the prostate, supporting the potential of SARMs for use in hormone replacement therapy.
[20][21] Estrogenic signaling in particular is essential for normal male physiology and health, including for instance maintenance of bone strength.
Conversely, in tissues where corepressors are in excess (such as prostate), SARMs act as partial agonists or antagonists.
Furthermore, each steroidal androgen or non-steroidal SARM uniquely influences distinct pathways depending on cell type.
[30] Due to their tissue selectivity, SARMs have the potential to treat a wide variety of conditions, including debilitating diseases.
They have been investigated in human studies for the treatment of osteoporosis, cachexia, benign prostatic hyperplasia, stress urinary incontinence, prostate cancer, and breast cancer and have also been considered for the treatment of Alzheimer's disease, Duchenne muscular dystrophy, hypogonadism and as a male contraceptive.
[19][7] As of 2023[update], there are no SARMs which have been approved for therapeutic use by the United States Food and Drug Administration or the European Medicines Agency.
[25] Enobosarm (ostarine) is the most well-studied SARM; according to its manufacturer, GTx Incorporated, 25 studies have been carried out on more than 1,700 humans as of 2020[update] involving doses from 1 to 18 mg each day.
[7][68] AAS were historically used successfully to treat AR positive breast cancer, but were phased out after the development of antiestrogen therapies, due to androgenic side effects and concerns about aromatization to estrogen (which does not occur with SARMs).
It is not known how SARMs interact with dietary protein intake and resistance training in people with muscle wasting.
[24][19] Phase II trials of enobosarm for stress urinary incontinence—considered promising, given that the levator ani muscle in the pelvic floor has a high androgen receptor density—did not meet their endpoint and were abandoned.
[19] In contrast to AAS and testosterone replacement, which have many side effects that have curtailed their medical use, SARMs are well tolerated and have mild and infrequent adverse events in randomized controlled trials.
[19][52] Several case reports have associated SARMs with hepatocellular drug-induced liver injury when used recreationally,[72] it is not known if the risk is significant for medical use.
[6][74][75] Marketing SARMs for human consumption is illegal in some jurisdictions and has led to criminal convictions in the United States[76] and the largest-ever fine levied under Australia's Therapeutic Goods Act 1989.
[6][79] SARMs are used by bodybuilders and competitive athletes due to their anabolic and lack of androgenic effects,[7] particularly in the United States, Europe, and other western countries.