Separated shoulder
[2][1] It is most commonly due to a fall onto the front and upper part of the shoulder when the arm is by the side.
[2] They are classified as type I, II, III, IV, V, or VI with the higher the number the more severe the injury.
[1] Separated shoulders often occur in people who participate in sports such as football, soccer, horseback riding, hockey, lacrosse, parkour, combat sports, rowing, rugby, snowboarding, skateboarding, crack the whip, cycling, roller derby and wrestling.
[citation needed] There are four types of soft tissue disruptions that may cause acromioclavicular separation:[8] Diagnosis is based on physical examination and an x-ray.
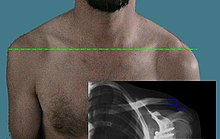
[citation needed] X-ray indicates a separated shoulder when the acromioclavicular joint space is widened (it is normally 5 to 8 mm).
A Type I AC separation involves direct trauma to the shoulder causing the injury to ligaments that form the joint, but no severe tearing or fracture.
[5] On radiographs, the lateral end of the clavicle may be slightly elevated by pressing on the sternal aspect of the clavicle forcing the acromial end down, and by releasing, it may pop back up eliciting a piano key sign due to the tearing of the AC.
In a Type III AC separation both acromioclavicular and coracoclavicular ligaments are torn without significant disruption of the deltoid or trapezial fascia.
[5] This is a more severe form of a type III injury, with the trapezial and deltoid fascia stripped off of the acromion as well as the clavicle.
[11] The humerus and scapula drop without having the clavicular strut to lift them, which manifests as a severely drooping shoulder.
[11] The mechanism is thought to be severe hyperabduction and external rotation of the arm, combined with retraction of the scapula.
Most patients with type VI injuries have paresthesia that resolves after relocation of the clavicle [11] It is extremely rare and generally only involved with motor vehicle collisions.
[citation needed] Most non-surgical treatment options include first immobilizing the arm with a sling for approximately 2 weeks followed by gradually improving shoulder movement using physical therapy to build up the muscles and help stabilize the joint.
[5] Literature regarding long-term follow-up after surgical repair of type III injuries is scarce, and those treated nonoperatively generally do quite well.
The strength training will include strengthening of the rotator cuff, and shoulder blade muscles.
Those who do have a separated shoulder will most often return to having full function, although some may have continued pain in the area of the AC joint.
[5] Medical device implants including coracoclavicular screws, a hook plate, fixation pins, and surgical wire may be necessary for repair of the joint.
[5] Many with type III shoulder separation who do not undergo surgical treatment recover just as well as those who do receive it, and avoid the added risks that surgery may present.
[5] Those with type III injuries who opt out of surgery often have faster recovery times, avoid hospitalization, and are able to return to work or sports sooner.
[5] Some studies suggest early surgical treatment of type III separation may benefit laborers and athletes who perform overhead motions.
[17] A common surgery is some form of modified Weaver-Dunn procedure, which involves cutting off the end of the clavicle portion, partially sacrificing the coracoacromial ligament and suturing the displaced acromial end to the lateral aspect of the clavicle for stabilization, then often some form of additional support is introduced to replace the coracoclavicular ligament(s).
Such exercises can include isometric strengthening which works the muscles without straining the healing of the joint.
[citation needed] Acromioclavicular joint dislocation is a common injury to the shoulder and is occurs most often in athletes.
[5] Amongst men, accidents or hits in sports such as boxing, football, ice hockey, and martial arts are the most common cause of this injury.