Shoulder
In human anatomy, the shoulder joint comprises the part of the body where the humerus attaches to the scapula, and the head sits in the glenoid cavity.
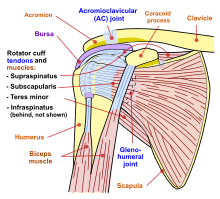
The shoulder consists of a ball-and-socket joint formed by the humerus and scapula and their surrounding structures - ligaments, muscles, tendons - which support the bones and maintain the relationship of one to another.
[1][2] These supporting structures attach to the clavicle, humerus, and scapula, the latter providing the glenoid cavity, acromion and coracoid processes.
Two filmy sac-like structures called bursae permit smooth gliding between bone, muscle, and tendon.
The "ball" of the joint is the rounded, medial anterior surface of the humerus and the "socket" is formed by the glenoid cavity, the dish-shaped portion of the lateral scapula.
The capsule is a soft tissue envelope that encircles the glenohumeral joint and attaches to the scapula, humerus, and head of the biceps.
This capsule is strengthened by the coracohumeral ligament which attaches the coracoid process of the scapula to the greater tubercle of the humerus.
[citation needed] The rotator cuff is an anatomical term given to the group of four muscles and their tendons that act to stabilize the shoulder.
[3] These muscles are the supraspinatus, infraspinatus, teres minor and subscapularis and that hold the head of the humerus in the glenoid cavity during movement.
The infraspinatus and the teres minor, along with the anterior fibers of the deltoid muscle, are responsible for external rotation of the arm.
[3] The nerves and blood vessels of the arm travel through the armpit, and it possesses several sets of lymph nodes that are able to be examined.
The shoulder can abduct, adduct, rotate, be raised in front of and behind the torso and move through a full 360° in the sagittal plane.
For all forms of rotator cuff tears, depending on the severity of the injury, possible treatments include rest, an arm sling, physical therapy, steroid injections, and non-steroidal anti-inflammatory drugs, or surgery.
[21] Imaging of the shoulder includes ultrasound, X-ray and MRI, and is guided by the suspected diagnosis and presenting symptoms.
Hodler et al. recommend starting scanning with conventional x-rays taken from at least two planes, since this method gives a wide first impression and even has the chance of exposing any frequent shoulder pathologies, i.e., decompensated rotator cuff tears, tendinitis calcarea, dislocations, fractures, usures, and/or osteophytes.
This method reveals:[26] The lateral contour of the shoulder should be positioned in front of the film in a way that the longitudinal axis of the scapula continues parallel to the path of the rays.
It is relatively cheap, does not emit any radiation, is accessible, is capable of visualizing tissue function in real time, and allows the performance of provocative maneuvers in order to replicate the patient’s pain.
One also has to have an extensive anatomical knowledge of the examined region and keep an open mind to normal variations and artifacts created during the scan.
[30] After the introduction of high-frequency transducers in the mid-1980s, ultrasound has become a conventional tool for taking accurate and precise images of the shoulder to support diagnosis.
Slow and cautious passive lateral and/or medial rotations have the effect of being able to visualize different sections of the shoulder.
In order to also demonstrate those parts which are hidden under the acromion in the neutral position, a maximum medial rotation with hyperextension behind the back is required.
[41] To accurately evaluate the echogenicity of an ultrasound, one has to take into account the physical laws of reflection, absorption and dispersion.
[43] MRIs can provide joint details to the treating orthopedist, helping them to diagnose and decide the next appropriate therapeutic step.
[44] While using MRI, true lesions at the rotator interval region between the parts of the supraspinatus and subscapularis are all but impossible to distinguish from normal synovium and capsule.
Through a fat suppressed T2-weighted spin echo, MRA can reproduce an extreme high fat-water-contrast, which helps to detect water-deposits with better damage diagnosis in structurally changed collagen fiber bundles.
Lacking a solid skeletal connection between the shoulder girdle and the vertebral column, the forelimb's attachment to the trunk is instead mainly controlled by serratus lateralis and levator scapulae.
In primates, the shoulder shows characteristics that differ from other mammals, including a well developed clavicle, a dorsally shifted scapula with prominent acromion and spine, and a humerus featuring a straight shaft and a spherical head.