Subthalamic nucleus
In humans there are also a small number (about 7.5%) of GABAergic interneurons that participate in the local circuitry; however, the dendritic arbors of subthalamic neurons shy away from the border and primarily interact with one another.
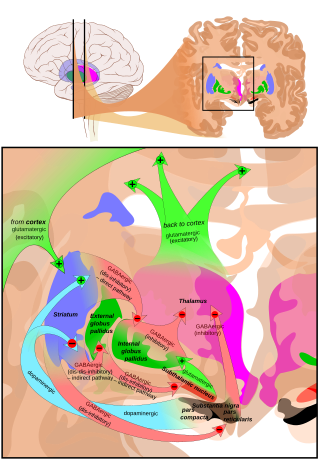
The subthalamic nucleus also receives neuromodulatory inputs, notably dopaminergic axons from the substantia nigra pars compacta.
Except for the connection to the striatum (17.3% in macaques), most of the subthalamic principal neurons are multitargets and directed to the other elements of the core of the basal ganglia.
[10][11] When all axons reaching this target are added, the main efference of the subthalamic nucleus is, in 82.7% of the cases, clearly the internal globus pallidus (GPi).
[citation needed] In these recordings three key observations were made, all three of which have dominated subsequent reports of subthalamic firing properties.
Oscillatory and synchronous activity[14][15] is likely to be a typical pattern of discharge in subthalamic neurons recorded from patients and animal models characterized by the loss of dopaminergic cells in the substantia nigra pars compacta, which is the principal pathology that underlies Parkinson's disease.
[21] This inspired Benazzouz and colleagues to probe deep brain stimulation of the nucleus, which was known to exert similar effects as ablative lesions.
[22] Soon after, the team of Alim Louis Benabid showed that deep brain stimulation of the nucleus leads to symptom relief in human patients with Parkinson disease, as well,[23] which led to the establishment of the currently FDA approved and widely applied form of deep brain stimulation.
In turn, adenosine A1 receptor activation depresses excitatory transmission in the thalamus, thus mimicking ablation of the subthalamic nucleus.
While this remains generally true, iatrogenic lesioning of the STN has been carried out numerous times and has recently gained new wind with the advent of MR guided focused ultrasound, which has also been probed for subthalamic nucleotomies to treat Parkinson disease.
[25] Curiously, a team around Michael Fox could recently show that, while some lesions that led to hemiballism were indeed in and around the STN, the majority of reported cases were in other regions of the brain.
[27] Application of high frequency pulses by deep brain stimulation has shown some promise in correcting severe impulsive behavior and has been FDA approved for treatment resistant cases with the disorder.
STN dysfunction has been implicated in motor symptoms such as rigidity, bradykinesia and tremor,[29] behavioral features such as stopping of ongoing movements[30] or impulsivity in individuals presented with two equally rewarding stimuli.