Anterior cruciate ligament injury
[5][6][7] While adults with a complete tear have a higher rate of later knee osteoarthritis, treatment strategy does not appear to change this risk.
[10] Risk factors include female anatomy, specific sports, poor conditioning, fatigue, and playing on a turf field.
Female athletes are more likely to jump and land with their knees relatively straight and collapsing in towards each other, while most of their bodyweight falls on a single foot and their upper body tilts to one side.
[citation needed] The ligament dominance theory suggests that when females athletes land after a jump, their muscles do not sufficiently absorb the impact of the ground.
[17] Female athletes are more likely to land with their upper body tilted to one side and more weight on one leg than the other, therefore placing greater rotational force on their knees.
[19] Governments and healthcare professionals acknowledge the high incidence of ACL injuries and have dedicated significant research efforts to prevention and rehabilitation.
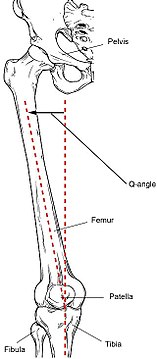
[24] The relatively wider female hip and widened Q angle may lead to an increased likelihood of ACL tears in women.
The tissue remodeling results in female ACLs that are smaller and will fail (i.e. tear) at lower loading forces, and differences in ligament and muscular stiffness between men and women.
Because of the elevated contraction of the quadriceps femoris muscle during physical activity, an increased strain is placed onto the ACL due to the "tibial translation anteriorly".
These bones are held together by ligaments, which are strong bands of tissue that keep the joint stable while an individual is walking, running, jumping, etc.
[28] In the anterior drawer test, the examiner flexes the knees to 90 degrees, sits on the person's feet, and gently pulls the tibia towards themself.
[31] Technological innovations like stop-action photography, force platforms, and programmable computers have propelled biomechanics into a key research area within the human sciences.
However, measuring force at joint, muscle, tendon, and articular surfaces, especially in the knee, is complex and relies heavily on intricate modeling of motion capture and medical imaging data.
This complexity has limited the involvement of biomechanists in designing, implementing, and evaluating prophylactic training interventions and neuromuscular rehabilitation programs.
[35] Another form of evaluation that may be used in case physical examination and MRI are inconclusive is laximetry testing (i.e. arthrometry and stress imaging), which involve applying a force to the leg and quantifying the resulting displacement of the knee.
The American Academy of Orthopedic Surgeons defines ACL injury in terms of severity and classifies them as Grade 1, 2, or 3 sprains.
[43][19] Injury prevention programs (IPPs), are reliable in reducing the risk factors of ACL inquiries, referring to dominance theories.
There is an increase in hip and knee flexion angles, such as plyometrics and jump-landing tasks, which reduces the risk of quadriceps dominance.
[44] One effective strategy to lower ACL injury risk is to enhance tissue strength, thereby improving its ability to withstand greater loads.
Surprisingly, there is a lack of published peer-reviewed studies showing that training can significantly increase strength in healthy ACL tissues through collagen regeneration.
[citation needed] Typically, this approach involves visiting a physical therapist or sports medicine professional soon after injury to oversee an intensive, structured program of exercises.
Non-surgical recovery typically takes three to six months, and depends on the extent of the original injury, pre-existing fitness and commitment to the rehabilitation and sporting goals.
Although there is no consensus on what rehab should consist of, some of the basic parameters include restoring range of motion, decreasing swelling, and ensuring there is adequate quadriceps strength.
[51] However, delaying ACL reconstruction in pediatric and adolescent populations for more than 3 months has been shown to increase the risk or meniscus injuries significantly.
[53] Asymmetry in the repaired knee is a possibility and has been found to have a large effect between limbs for peak vertical ground reaction force, peak knee-extension moment, and loading rate during double-limb landings, as well as mean knee-extension moment and knee energy absorption during both double- and single-limb landings.
If an individual with an ACL injury undergoes surgery, the rehabilitation process will first focus on slowly increasing the range of motion of the joint, then on strengthening the surrounding muscles to protect the new ligament and stabilize the knee.
More than half of physical therapists still utilize manual muscle testing techniques to measure leg strength for return to sports which is subjective and not reliable data.
A Guideline Development Group (GDG), composed of impartial clinical and methodology experts, was formed and tasked with converting evidence into recommendations.
[64] Therefore, athletes should be screened for any neuromuscular deficit (i.e. weakness greater in one leg than another, or incorrect landing form) before returning to sport.
A study of insurance data showed the majority of the breeds with increased risk of cruciate ligament rupture were large or giant.