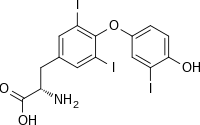
Triiodothyronine
[1] Production of T3 and its prohormone thyroxine (T4) is activated by thyroid-stimulating hormone (TSH), which is released from the anterior pituitary gland.
This pathway is part of a closed-loop feedback process: Elevated concentrations of T3, and T4 in the blood plasma inhibit the production of TSH in the anterior pituitary gland.
[2] T3 helps deliver oxygen and energy to all of the body's cells, its effects on target tissues being roughly four times more potent than those of T4.
T4 is deiodinated by three deiodinase enzymes to produce the more-active triiodothyronine: T4 is synthesised in the thyroid follicular cells as follows.
[8] T3 and T4, although being lipophilic, are not able to passively diffuse through the phospholipid bilayers of target cells,[9] instead relying on transmembrane iodothyronine transporters.
The thyroid receptors bind to response elements in gene promoters, thus enabling them to activate or inhibit transcription.
The saturation of binding spots on thyronine-binding globulin (TBG) by endogenous T3 can be estimated by the triiodothyronine resin uptake test.
The test is performed by taking a blood sample, to which an excess of radioactive exogenous T3 is added, followed by a resin that also binds T3.
The basal metabolic rate is the minimal caloric requirement needed to sustain life in a resting individual.
It increases the synthesis and activity of the Na+/K+-ATPase (which normally constitutes a substantial fraction of total cellular ATP expenditure) without disrupting transmembrane ion balance.
[18] The addition of triiodothyronine to existing treatments such as SSRIs is one of the most widely studied augmentation strategies for refractory depression,[19] however success may depend on the dosage of T3.
[19] The same authors published a retrospective study of 125 patients with the two most common categories of bipolar disorders II and NOS whose treatment had previously been resistant to an average of 14 other medications.
Several studies have shown that these compounds increase the metabolization of fatty acids and the burning of adipose fat tissue in rats.
The American Thyroid Association has raised concern that the prescribed treatment with triiodothyronine is potentially harmful.
[23] In 1950 Dr Jack Gross, a Canadian endocrinologist, came to the British National Institute for Medical Research to work with Rosalind Pitt-Rivers as a postdoctoral fellow.
Around that time a group led by Jean Roche in Paris described a deiodinating activity in the sheep thyroid gland, raising the possibility that 'unknown 1' is the less iodinated analogue of T4, triiodothyronine.
[25] While Gross & Pitt-Rivers are normally credited with discovering T3, this compound was actually first isolated by the biochemists Hird & Trikojus at the University of Melbourne in 1948.