Cauda equina syndrome
[1][2] The diagnosis is suspected based on symptoms and confirmed by medical imaging such as MRI or CT scan.
[1] Sudden onset is regarded as a medical emergency requiring prompt surgical decompression, with delay causing permanent loss of function.
[5] Signs and symptoms of cauda equina syndrome include: Severe back pain, saddle anesthesia, urinary or fecal incontinence and sexual dysfunction are considered "red flags", i.e. features which require urgent investigation.
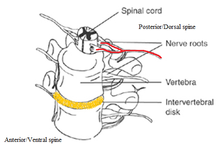
Compression, trauma or other damage to this region of the spinal canal can result in cauda equina syndrome.
[10] Cauda equina syndrome may also be caused by blunt trauma suffered in an event such as a car accident or fall.
Race has little influence with the notable exception that African Americans appear slightly less likely to develop CES than other groups.
[citation needed] Early surgery in acute onset of severe cases has been reported to be important.
[citation needed] The management of true cauda equina syndrome frequently involves surgical decompression.
When cauda equina syndrome is caused by a herniated disk early surgical decompression is recommended.
[4] Surgical decompression by means of laminectomy or other approaches may be undertaken within 6,[18] 24[19] or 48 hours of symptoms developing if a compressive lesion (e.g., ruptured disc, epidural abscess, tumor or hematoma) is demonstrated.
If the syndrome is due to an inflammatory condition e.g., ankylosing spondylitis, anti-inflammatory, including steroids can be used as an effective treatment.
Issues could include the person's need for physiotherapy and occupational therapy due to lower limb dysfunction.
[full citation needed] These exercises can be done standing, lying, or on all fours with the knees slightly separated.
[citation needed] Review of the literature indicates that around 50–70% of patients have urinary retention (CES-R) on presentation with 30–50% having an incomplete syndrome (CES-I).
[23] Various etiologies of CES include fractures, abscesses, hematomas, and any compression of the relevant nerve roots.
Few epidemiological studies of CES have been done in the United States, owing to difficulties such as amassing sufficient cases as well as defining the affected population, therefore this is an area deserving of additional scrutiny.
[12][13]CES is often concurrent with congenital or degenerative diseases and represents a high cost of care to those admitted to the hospital for surgery.
[26] Delays in care for cauda equina results in the English NHS paying about £23 million a year in compensation.