Shock (circulatory)
Shock is the state of insufficient blood flow to the tissues of the body as a result of problems with the circulatory system.
Initial symptoms of shock may include weakness, tachycardia, hyperventilation, sweating, anxiety, and increased thirst.
While waiting for medical care, the individual should be, if safe, laid down (except in cases of suspected head or back injuries).
[6] While the general signs for all types of shock are low blood pressure, decreased urine output, and confusion, these may not always be present.
Dry mucous membrane, reduced skin turgor, prolonged capillary refill time, weak peripheral pulses, and cold extremities can be early signs of shock.
As such, shock is a runaway condition of homeostatic failure, where the usual corrective mechanisms relating to oxygenation of the body no longer function in a stable way.
When it occurs, immediate treatment is critical in order to return an individual's metabolism into a stable, self-correcting trajectory.
The baroreceptors in the arteries detect the hypotension resulting from large amounts of blood being redirected to distant tissues, and cause the release of epinephrine and norepinephrine.
The renin–angiotensin axis is activated, and arginine vasopressin (anti-diuretic hormone) is released to conserve fluid by reducing its excretion via the renal system.
These hormones cause the vasoconstriction of the kidneys, gastrointestinal tract, and other organs to divert blood to the heart, lungs and brain.
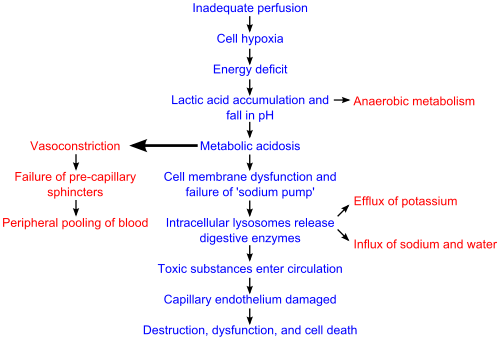
As anaerobic metabolism continues, the arteriolar smooth muscle and precapillary sphincters relax such that blood remains in the capillaries.
[18] Due to this, the hydrostatic pressure will increase and, combined with histamine release, will lead to leakage of fluid and protein into the surrounding tissues.
[18] If the bowel becomes sufficiently ischemic, bacteria may enter the blood stream, resulting in the increased complication of endotoxic shock.
One of the primary reasons that shock is irreversible at this point is that much of the cellular ATP (the basic energy source for cells) has been degraded into adenosine in the absence of oxygen as an electron receptor in the mitochondrial matrix.
Adenosine easily perfuses out of cellular membranes into extracellular fluid, furthering capillary vasodilation, and then is transformed into uric acid.
[25] The diagnosis of shock is commonly based on a combination of symptoms, physical examination, and laboratory tests.
Mixed venous oxygen saturation (SmvO2) is one of the methods of calculating cardiac output with a pulmonary artery catheter.
[3] In the United States about 1.2 million people present to the emergency room each year with shock and their risk of death is between 20 and 50%.
[9] Management may include securing the airway via intubation if necessary to decrease the work of breathing and for guarding against respiratory arrest.
[28] It is important to keep the person warm to avoid hypothermia[29] as well as adequately manage pain and anxiety as these can increase oxygen consumption.
[22] Aggressive intravenous fluids are recommended in most types of shock (e.g. 1–2 liter normal saline bolus over 10 minutes or 20 mL/kg in a child) which is usually instituted as the person is being further evaluated.
[32] If the person remains in shock after initial resuscitation, packed red blood cells should be administered to keep the hemoglobin greater than 100 g/L.
There is no evidence of substantial benefit of one vasopressor over another;[36] however, using dopamine leads to an increased risk of arrhythmia when compared with norepinephrine.
[20] Activated protein C (Xigris), while once aggressively promoted for the management of septic shock, has been found not to improve survival and is associated with a number of complications.
Low volume, anaphylactic, and neurogenic shock are readily treatable and respond well to medical therapy.
[45] Shock or "choc" was first described in a trauma victim in the English translation of Henri-François LeDran's 1740 text, Traité ou Reflexions Tire'es de la Pratique sur les Playes d'armes à feu (A treatise, or reflections, drawn from practice on gun-shot wounds.
[47] Other competing theories around the turn of the century included one penned by Malcom in 1907, in which the assertion was that prolonged vasoconstriction led to the pathophysiological signs and symptoms of shock.