Glycated hemoglobin
[note 1] Most monosaccharides, including glucose, galactose, and fructose, spontaneously (that is, non-enzymatically) bond with hemoglobin when they are present in the bloodstream.
[5] HbA1c is measured primarily to determine the three-month average blood sugar level and is used as a standard diagnostic test for evaluating the risk of complications of diabetes and as an assessment of glycemic control.
[11] Its increase in diabetes was first described in 1969 by Samuel Rahbar et al.[12] The reactions leading to its formation were characterized by Bunn and his coworkers in 1975.
[13] The use of hemoglobin A1c for monitoring the degree of control of glucose metabolism in diabetic patients was proposed in 1976 by Anthony Cerami, Ronald Koenig, and coworkers.
[15] Another way glycated hemoglobin causes damage is via inflammation, which results in atherosclerotic plaque (atheroma) formation.
[15] Highly glycated Hb-AGEs go through vascular smooth muscle layer and inactivate acetylcholine-induced endothelium-dependent relaxation, possibly through binding to nitric oxide (NO), preventing its normal function.
NO is a potent vasodilator and also inhibits formation of plaque-promoting LDLs (sometimes called "bad cholesterol") oxidized form.
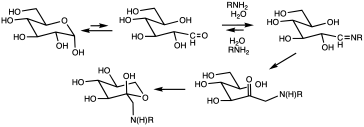
[15] Glycation of proteins is a frequent occurrence, but in the case of hemoglobin, a nonenzymatic condensation reaction occurs between glucose and the N-end of the beta chain.
Measuring glycated hemoglobin assesses the effectiveness of therapy by monitoring long-term serum glucose regulation.
[19] This is also supported by data from clinical practice showing that HbA1c levels improved significantly after 20 days from start or intensification of glucose-lowering treatment.
Conversion between DCCT and IFCC is by the following equation:[27] Laboratory results may differ depending on the analytical technique, the age of the subject, and biological variation among individuals.
[28] Results from large trials in 2008–09 suggested that a target below 53 mmol/mol (7.0 DCCT %) for older adults with type 2 diabetes may be excessive: Below 53 mmol/mol, the health benefits of reduced A1c become smaller, and the intensive glycemic control required to reach this level leads to an increased rate of dangerous hypoglycemic episodes.
[citation needed] Persistent elevations in blood sugar (and, therefore, HbA1c) increase the risk of long-term vascular complications of diabetes, such as coronary disease, heart attack, stroke, heart failure, kidney failure, blindness, erectile dysfunction, neuropathy (loss of sensation, especially in the feet), gangrene, and gastroparesis (slowed emptying of the stomach).
Higher target values are appropriate for children and adolescents, patients with extensive co-morbid illness and those with a history of severe hypoglycemia.
For these patients, alternate assessment with fructosamine or glycated albumin is recommended; these methods reflect glycemic control over the preceding 2-3 weeks.
Since these new RBCs will have only existed for a short period of time, their presence will lead HbA1c to underestimate the actual average levels.
[44] HbA1c levels show a small, but statistically significant, progressive uptick with age; the clinical importance of this increase is unclear.
[49] Due to glycated hemoglobin's variability (as shown in the table above), additional measures should be checked in patients at or near recommended goals.
Continuous use of blood glucose monitors is becoming more common, and the devices are covered by many health insurance plans, including Medicare in the United States.
The thiobarbituric acid method (a chemical method specific for the detection of glycation) shows that patients with kidney failure have values for glycated hemoglobin similar to those observed in normal subjects, suggesting that the high values in these patients are a result of binding of something other than glucose to hemoglobin.
[51] The alternative fructosamine test may be used in these circumstances and it also reflects an average of blood glucose levels over the preceding 2 to 3 weeks.
[36] Analytical performance has been a problem with earlier point-of-care devices for HbA1c testing, specifically large standard deviations and negative bias.