Hodgkin lymphoma
[5] About half of cases of Hodgkin lymphoma are due to Epstein–Barr virus (EBV) and these are generally the classic form.
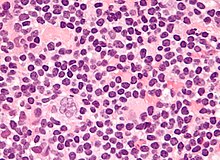
[2][3] Diagnosis is conducted by confirming the presence of cancer and identifying RS cells in lymph node biopsies.
After Hodgkin lymphoma is diagnosed, a person will be staged: that is, they will undergo a series of tests and procedures that will determine what areas of the body are affected.
These procedures may include documentation of their histology, a physical examination, blood tests, chest X-ray radiographs, computed tomography (CT)/positron emission tomography (PET)/magnetic resonance imaging (MRI) scans of the chest, abdomen and pelvis, and usually a bone marrow biopsy.
On the PET scan, sites involved with lymphoma light up very brightly enabling accurate and reproducible imaging.
[35] In the past, a lymphangiogram or surgical laparotomy (which involves opening the abdominal cavity and visually inspecting for tumors) were performed.
[39] Characteristics of classic Reed–Sternberg cells include large size (20–50 micrometres), abundant, amphophilic, finely granular/homogeneous cytoplasm; two mirror-image nuclei (owl eyes) each with an eosinophilic nucleolus and a thick nuclear membrane (chromatin is distributed close to the nuclear membrane).
[42] The current approach for treatment aims to reduce the acute and long-term toxicities associated with Hodgkin lymphoma (e.g. cardiac damage and secondary cancers) and increase overall survival.
[43] People with early stage disease (IA or IIA) can be treated effectively with radiation therapy or chemotherapy.
[45] Although no longer the most effective combination, MOPP is still used after relapse or where the person has certain allergies or lung or heart problems which prevents the use of another regimen.
The common non-Hodgkin treatment, rituximab (which is a monoclonal antibody against CD20) is not routinely used to treat Hodgkin lymphoma due to the lack of CD20 surface antigens in most cases.
[51][52] Recently, two novel targeted drugs have been developed for relapsing and refractory HL patients; Brentuximab vedotin, a CD30 antibody conjugated with a cytotoxic component MMAE,[53] and the checkpoint inhibitors, Nivolumab and Pembrolizumab.
Total nodal irradiation is when the therapist gives radiation to all the lymph nodes in the body to destroy cells that may have spread.
[59] The high cure rates and long survival of many people with Hodgkin lymphoma has led to a high concern with late adverse effects of treatment, including cardiovascular disease and second malignancies such as acute leukemias, lymphomas, and solid tumors within the radiation therapy field.
Clinical research strategies are exploring reduction of the duration of chemotherapy and dose and volume of radiation therapy in an attempt to reduce late morbidity and mortality of treatment while maintaining high cure rates.
[60] In childhood cases of Hodgkin lymphoma, long-term endocrine adverse effects are a major concern, mainly gonadal dysfunction and growth retardation.
Gonadal dysfunction seems to be the most severe endocrine long-term effect, especially after treatment with alkylating agents or pelvic radiotherapy.
[66] In 1998, an international effort[67] identified seven prognostic factors that accurately predict the success rate of conventional treatment in people with locally extensive or advanced-stage Hodgkin lymphoma.
[68] The adverse prognostic factors identified in the international study are: Other studies have reported the following to be the most important adverse prognostic factors: mixed-cellularity or lymphocyte-depleted histologies, male sex, large number of involved nodal sites, advanced stage, age of 40 years or more, the presence of B symptoms, high erythrocyte sedimentation rate, and bulky disease (widening of the mediastinum by more than one third, or the presence of a nodal mass measuring more than 10 cm in any dimension.
)[69] More recently, the use of positron emission tomography (PET) early after commencing chemotherapy has demonstrated to have powerful prognostic ability.
[70] This enables assessment of an individual's response to chemotherapy as the PET activity switches off rapidly in people who are responding.
Several trials are underway to see if PET-based risk adapted response can be used to improve a person's outcomes by changing chemotherapy early in people who are not responding.
Negative interim PET scan results probably result in a large increase in the overall survival compared to those with a positive interim PET scan result,[43] Unlike some other lymphomas, whose number of new cases per year increases with age, Hodgkin lymphoma has a bimodal curve for the number of cases; that is, it occurs most frequently in two separate age groups, the first being young adulthood (age 15–35) and the second being in those over 55 years old although these peaks may vary slightly with nationality.
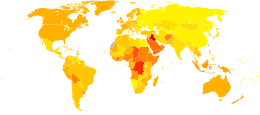
The annual number of cases of Hodgkin lymphoma is 2.7 per 100,000 per persons per year, and the disease accounts for slightly less than 1% of all cancers worldwide.
[74] The East Mediterranean Region also has the highest age-standardized mortality rate of 1.0 per 100,000, which is mainly attributed to lifestyle and environmental risk factors associated with transitional economies such as smoking, obesity, physical inactivity, and reproductive behaviors, as well as availability of diagnostic practices and awareness of the disease.
[75] In contrast to many other lymphomas associated with HIV infection it occurs most commonly in people with higher CD4 T cell counts.
[79][10] While occupied as museum curator at Guy's Hospital, London, Hodgkin studied seven people with painless lymph node enlargement.
[79] Carswell's report of the seventh case was accompanied by numerous illustrations that aided early descriptions of the disease.