Lower respiratory tract infection
[citation needed] Antibiotics are the first line treatment for pneumonia; however, they are neither effective nor indicated for parasitic or viral infections.
[7] Acute exacerbations of chronic bronchitis (AECB) are frequently due to non-infective causes along with viral ones.
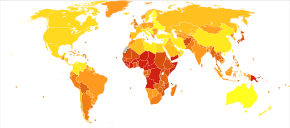
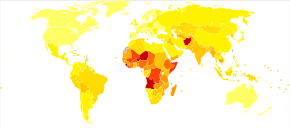
[13][15] Pneumonia is also the leading cause of death in children less than five years of age in low income countries.
[14] For optimal management of a pneumonia patient, the following must be assessed: pneumonia severity (including treatment location, e.g., home, hospital or intensive care), identification of causative organism, analgesia of chest pain, the need for supplemental oxygen, physiotherapy, hydration, bronchodilators and possible complications of emphysema or lung abscess.
[19] Specifically for the children with low serum retinol or who are suffering from malnutrition, vitamin A supplements are recommended as a preventive measure against acute LRTI.
[22] The treatment of bacterial pneumonia is selected by considering the age of the patient, the severity of the illness and the presence of underlying disease.
[21] Another cochrane review suggests that new studies are needed to confirm that azithromycin may lead to less treatment failure and lower side effects than amoxycillin.
[24] In the other hand, there is no sufficient evidence to consider the antibiotics as a prophylaxis for the high risk children under 12 years.
[26] For children younger than 15 years old, nasopharyngel catheters or nasal prongs are recommended over a face mask or head box.
[26] A Cochrane review in 2014 presented a summary to identify children complaining of severe LRTI, however; further research is required to determine the effectiveness of supplemental oxygen and the best delivery method.
[citation needed] Workplace burdens arise from the acquisition of a lower respiratory tract infection, with factors such as total per person expenditures and total medical service utilisation demonstrated as greater among individuals experiencing a lower respiratory tract infection.