Signs and symptoms of multiple sclerosis
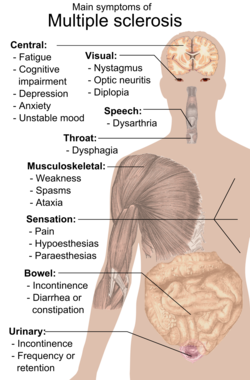
Multiple sclerosis can cause a variety of symptoms varying significantly in severity and progression among individuals: changes in sensation (hypoesthesia), muscle weakness, abnormal muscle spasms, or difficulty moving; difficulties with coordination and balance; problems in speech (dysarthria) or swallowing (dysphagia), visual problems (nystagmus, optic neuritis, phosphenes or diplopia), fatigue and acute or chronic pain syndromes, bladder and bowel difficulties, cognitive impairment, or emotional symptomatology (mainly major depression).
The most common initial symptoms reported are: changes in sensation in the arms, legs or face (33%), complete or partial vision loss (optic neuritis) (20%), weakness (13%), double vision (7%), unsteadiness when walking (5%), and balance problems (3%); but many rare initial symptoms have been reported such as aphasia or psychosis.
[41] A 2024 study found results suggested that fatigue was not driven by neuroinflammation or neurodegeneration measurable by current structural MRI in early RRMS.
[42] Medications used to treat MS fatigue include amantadine,[43][44] pemoline,[45][46] methylphenidate, and modafinil,[47] as well as cognitive behavioral therapy (CBT) and psychological interventions of energy conservation;[48][49] but their effects are limited.
[50] Bladder problems (See also urinary system and urination) appear in 70–80% of people with multiple sclerosis (MS) and they have an important effect both on hygiene habits and social activity.
Pharmacological treatments vary greatly depending on the origin or type of dysfunction and some examples of the medications used are:[55] alfuzosin for retention,[56] trospium and flavoxate for urgency and incontinency,[57][58] and desmopressin for nocturia.
[59][60] Non pharmacological treatments involve the use of pelvic floor muscle training, stimulation, biofeedback, pessaries, bladder retraining, and sometimes intermittent catheterization.
[62][63] Some of the most common deficits affect recent memory, attention, processing speed, visual-spatial abilities and executive function.
[65] Cognitive impairments occur in about 40 to 60 percent of patients with multiple sclerosis,[71][72] [67] with the lowest percentages usually from community-based studies and the highest ones from hospital-based.
[68] Neuropsychological rehabilitation may help to reverse or decrease the cognitive deficits although studies on the issue have been of low quality.
[citation needed] Clinical depression is the most common neuropsychiatric condition: lifetime depression prevalence rates of 40–50% and 12-month prevalence rates around 20% have been typically reported for samples of people with MS; these figures are considerably higher than those for the general population or for people with other chronic illnesses.
This results in the failure of the medial rectus muscle to contract appropriately, so that the eyes do not move equally (called disconjugate gaze).
Within five years of onset the EDSS is six in 50% of those with the progressive form of MS.[87] A wide range of impairments may exist in people with MS, which can act either alone or in combination to impact directly on a person's balance, function and mobility.
This second level intervention includes provision, education, and instruction in the use of equipment such as walking aids, wheelchairs, motorized scooters and car adaptations as well as instruction on compensatory strategies to accomplish an activity — for example undertaking safe transfers by pivoting in a flexed posture rather than standing up and stepping around.
The presence of demyelinating white matter lesions on brain MRIs at the time of presentation for optic neuritis is the strongest predictor in developing clinical diagnosis of MS.
[citation needed] A systemic intravenous treatment with corticosteroids may quicken the healing of the optic nerve, prevent complete loss of vision and delay the onset of other symptoms.
[103] Subacute pain is usually secondary to the disease and can be a consequence of spending too much time in the same position, urinary retention, or infected skin ulcers.
[109][110] Lhermitte's sign is an electrical sensation that runs down the back and into the limbs and is produced by bending the neck forward.
The abnormal sensations are caused by lesions of the peripheral or central sensory pathways, and are described as painful feelings such as burning, wetness, itching, electric shock or pins and needles.
[121] Erectile dysfunction appears to be the most common form of SD documented in MS. SD may be due to alteration of the ejaculatory reflex which can be affected by neurological conditions such as MS.[121] Sexual dysfunction is also prevalent in female MS patients, typically lack of orgasm, probably related to disordered genital sensation.
[125] There is evidence, albeit limited, of the clinical effectiveness of THC and CBD extracts,[126] baclofen,[127] dantrolene,[128] diazepam,[129] and tizanidine.
[137] Some MS patients develop rapid onset of numbness, weakness, bowel or bladder dysfunction, and/or loss of muscle function, typically in the lower half of the body.
[citation needed] Though it was considered for many years that traverse myelitis was a normal consequence of MS, since the discovery of anti-AQP4 and anti-MOG biomarkers it is not.
It is the most common of all involuntary movements and can affect the hands, arms, head, face, vocal cords, trunk, and legs.
Ataxia is an unsteady and clumsy motion of the limbs or torso due to a failure of the gross coordination of muscle movements.
People with ataxia experience a failure of muscle control in their arms and legs, resulting in a lack of balance and coordination or a disturbance of gait.
[139] The origin of tremor in MS is difficult to identify but it can be due to a mixture of different factors such as damage to the cerebellar connections, weakness, spasticity, etc.
Medications that have been reported to provide some relief are isoniazid,[140][141][142][143] carbamazepine,[104] propranolol[144][145][146] and gluthetimide[147] but published evidence of effectiveness is limited.
Rather it is regarded as a secondary effect resulting from other factors that are themselves caused or exacerbated by MS, such as spasms, pain, anxiety, depression and high caffeine intake.
[158] CPAP treatment in patients with MS and sleep apnea may reduce fatigue and improve the physical quality of life.