Tympanostomy tube
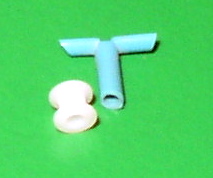
[1] The tube itself is made in a variety of designs, most often shaped like a grommet for short-term use, or with long flanges and sometimes resembling a T-shape for long-term use.
Options for use in adults include: Otorrhea (ear discharge) is the most common complication of tympanostomy tube placement, affecting between 25–75% of children receiving this procedure.
After two weeks children do not need to wear earplugs when swimming or to take other measures to prevent water from getting in their ears as there is minimal reduction in adverse effects.
[1] The eardrum usually closes without a residual hole at the tube site but in a small number of cases a perforation can persist.
There is consensus, however, on the beneficial role of tympanostomy tubes in allowing for drainage of infections and offering direct access to the middle ear with antibiotic drops.
[1][6] The first myringotomy dates back to 1649 when French anatomist Jean Riolan noticed an improvement in his hearing after intentionally perforating his eardrum with a spoon.
These scientists used an approximately 6mm long gold tube in an attempt to prevent the eardrum from closing after myringotomy.
[18] From 1845 to 1875, seven different types of tympanostomy tubes were manufactured and made of materials including rubber, silver, aluminum, and gold.
[18] In 1952, tympanostomy tubes would make a return when American otolaryngologist Beverly Armstrong introduced them as a new treatment for chronic secretory otitis media.