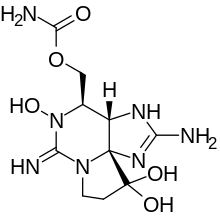
Neosaxitoxin
[3] NSTX, and other PSTs, are produced by several species of marine dinoflagellates (eukaryotes) and freshwater cyanobacteria, blue-green algae (prokaryotes), which can form extensive blooms around the world.
[22] This mechanism of action can produce two well known kinds of effects in humans: It can be approximately described using one of the classical model of neurotoxic disease, known from ancient times as red tide, the most harmful algal bloom (HAB).
[23] Of course, there are great differences between different algal blooms,[24][25][26][27] because of the mix of species included in each HAB, usually related to environmental conditions;[28] because of the levels and quality of PSTs produced in each HAB, that may be modulated by concurrent microorganism;[29][30][31][32] and, last but not least, because of the specific properties of each kind of PST, for example: In spite of its heterogeneous and poorly understood epidemiology, the clinical picture of PSP could be useful to anticipate clinical effects of systemic NSTX.
Usually, the victims of mild and severe acute intoxications eliminate the toxin in urine during the first 24 hours after ingestion, and improve to full recovery in the first day of intrahospital care (when vital support is provided in a timely manner).
[40] When outbreaks of PSP occur in remote locations, where medical assistance is limited, reported lethality is under 10% in adults, but can reach 50% in children younger than six years old.
Some evidence suggest the presence of metabolic pathways for the sequential oxidation and glucuronidation of PST in vitro, both being the initial detoxication reactions for the excretion of these toxins in humans.
[46] Forensic analysis of fatalities after severe cases, conclude that PSP toxins are metabolically transformed by humans and that they are removed from the body by excretion in the urine and feces like any other xenobiotic compound.
[51][52] One study in rats exposed to chronic (12 weeks) NSTX administration demonstrated some reduction in water and food intake, and a mild degree of transient cholestasis, probably associated to fasting, without other abnormalities.