Neuroanatomy of memory
Also, there is evidence that experience in building extensive mental maps, such as driving a city taxi for a long time (since this requires considerable memorization of routes), can increase the volume of one's hippocampus.
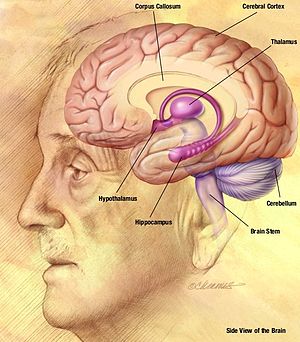
[2] Damage to the hippocampus and surrounding area can cause anterograde amnesia, the inability to form new memories.
[4] An example of a skill requiring procedural memory would be playing a musical instrument, or driving a car or riding a bike.
[7] This may be due to the amygdala enhancing the emotional aspect of the information during encoding, causing the memory to be processed at a deeper level and therefore, more likely to withstand forgetting.
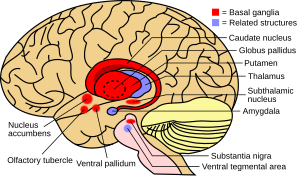
The basal ganglia are a group of nuclei which are located in the medial temporal lobe, above the thalamus and connected to the cerebral cortex.
[4] Particularly, one division within the ventral striatum, the nucleus accumbens core, is involved in the consolidation, retrieval and reconsolidation of drug memory.
[9] The caudate nucleus is thought to assist in learning and memory of associations taught during operant conditioning.
Specifically, research has shown that this part of the basal ganglia plays a role in acquiring stimulus-response habits, as well as in solving sequence tasks.
Most disorders that are associated with damage to these areas of the brain involve some type of motor dysfunction, as well as trouble with mental switching between tasks in working memory.
It is separated from the parietal lobe by the primary motor cortex, which controls voluntary movements of specific body parts associated with the precentral gyrus.
[10] The cortex here serves our ability to plan the day, organize work, type a letter, pay attention to details and control the movements of your arms and legs.
[13] The temporal lobes are a region of the cerebral cortex that is located beneath the Sylvian fissure on both the left and right hemispheres of the brain.
[19] The parietal lobe helps us to mediate attention when necessary and provides spatial awareness and navigational skills.
[20] Damage to the parietal lobe results in the syndrome ‘neglect' which is when patients treat part of their body or objects in their visual field as though it never existed.
Right side damage can also cause difficulty in making things (constructional apraxia), denial of deficits (anosognosia) and drawing ability.
[21] Neglect syndrome tends to be more prevalent on the right side of the parietal lobe, because the right mediates attention to both the left and right fields.
[21] Damage in the somatic sensory cortex results in loss of perception of bodily sensations, namely sense of touch.
Once the Lateral Geniculate Nucleus receives the information it is sent down the primary visual cortex where it is organized and sent down one of two possible path ways; dorsal or ventral stream.
[19] A study was done in which patients suffered from a tumour on the occipital lobe and the results shows that the most frequent consequence was contralateral damage to the visual field.
Damage to the left side of the brain can lead to language discrepancies, i.e. difficulty in properly identifying letters, numbers and words, inability to incorporate visual stimuli to comprehend multiple ways an object can be found.
[19] Right side damage causes non-verbal problems, i.e. identifying geometric shapes, perception of figures and faces.
In one study, FTLD patients were interviewed and asked to describe a significant event from five different periods of their lives.
[24] Through image processing, patterns of significant reduced parenchymal volumes that encompass the frontal and temporal lobes were found.
[25] Most people can instantly and easily use visual-spatial memory to remember locations and pictures, but a person with Parkinson's disease would find this difficult.