Neuroendocrine tumor
Although there are many kinds of NETs, they are treated as a group of tissue because the cells of these neoplasms share common features, including a similar histological appearance, having special secretory granules, and often producing biogenic amines and polypeptide hormones.
Tumor necrosis, although recognized as a factor associated with a potentially worse prognosis, is not included in the grading of NETs of the gastrointestinal or pancreaticobiliary tract.
However, the absence or presence of tumor necrosis is a component of the grading of NETs of many other origins, such as the upper aerodigestive tract, the lung and the thymus.
[7] Furthermore, the 2022 WHO classification introduces a two-tiered grading system for medullary thyroid carcinomas based on mitotic count, Ki-67 index and the absence or presence of tumor necrosis.
[citation needed] It has been proposed that the current G3 category be further separated into histologically well-differentiated and poorly-differentiated neoplasms to better reflect prognosis.
[52] The excessive outflow of serotonin can cause a depletion of tryptophan leading to niacin deficiency, and thus pellagra,[1] which is associated with dermatitis, dementia, and diarrhea.
Bowel obstruction can occur, sometimes due to fibrosing effects of NET secretory products[49] with an intense desmoplastic reaction at the tumor site, or of the mesentery.
Up to 60% of PanNETs are nonsecretory or nonfunctional, which either don't secrete, or the quantity or type of products such as pancreatic polypeptide (PPoma), chromogranin A, and neurotensin do not cause a clinical syndrome, although blood levels may be elevated.
[citation needed] In addition to the two main categories of GEP-NET, there are rarer forms of neuroendocrine tumors that arise anywhere in the body, including within the lung, thymus and parathyroid.
Bronchial carcinoid can cause airway obstruction, pneumonia, pleurisy, difficulty with breathing, cough, and hemoptysis, or may be associated with weakness, nausea, weight loss, night sweats, neuralgia, and Cushing's syndrome.
[60] Given the diverse secretory activity of NETs there are many other potential markers, but a limited panel is usually sufficient for clinical purposes.
While MRI is generally superior to CT, both for detection of the primary tumor and for evaluation of metastases, CECT is more widely available, even at academic institutions.
Functional imaging with gallium-labelled somatostatin analog and 18F-FDG PET tracers ensures better staging and prognostication of neuroendocrine neoplasms.
[66] The ability to perform this as a whole body study is highlighting the limitations of relying on histopathology obtained from a single site.
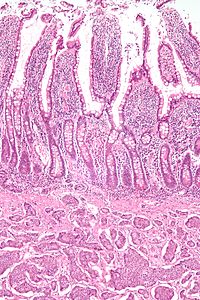
[71] NETs are often small, yellow or tan masses, often located in the submucosa or more deeply intramurally, and they can be very firm due to an accompanying intense desmoplastic reaction.
[citation needed] NETs from a particular anatomical origin often show similar behavior as a group, such as the foregut (which conceptually includes pancreas, and even thymus, airway and lung NETs), midgut and hindgut; individual tumors within these sites can differ from these group benchmarks:[citation needed] Several issues help define appropriate treatment of a neuroendocrine tumor, including its location, invasiveness, hormone secretion, and metastasis.
If the tumor is locally advanced or has metastasized, but is nonetheless slowly growing, treatment that relieves symptoms may often be preferred over immediate challenging surgeries.
[citation needed] Intermediate and high grade tumors (noncarcinoids) are usually best treated by various early interventions (active therapy) rather than observation (wait-and-see approach).
Similarly, recent advances in understanding neuroendocrine tumor's molecular and genomic alterations still have to find their ways into a definitive management strategy.
[83]: 46 In secretory tumors, somatostatin analogs given subcutaneously or intramuscularly alleviate symptoms by blocking hormone release.
In this study, lanreotide showed a statistically significant improvement in progression-free survival, meeting its primary endpoint.
[86] Lanreotide is the first and only FDA approved antitumor therapy demonstrating a statistically significant progression-free survival benefit in a combined population of patients with GEP-NETS.
[88] Most gastrointestinal carcinoid tumors tend not to respond to chemotherapy agents,[52] showing 10 to 20% response rates that are typically less than 6 months.
Combining chemotherapy medications has not usually been of significant improvement[52] showing 25 to 35% response rates that are typically less than 9 months.
[1] Targeted therapy with everolimus (Afinitor) and sunitinib (Sutent) is approved by the FDA in unresectable, locally advanced or metastatic PanNETs.
Although marginally effective in well-differentiated PETs, cisplatin with etoposide is active in poorly differentiated neuroendocrine cancers (PDNECs).
[49][93] AdVince, a type of gene therapy using a genetically modified oncolytic adenovirus[97] and supported by the crowdfunding campaign iCancer[98] was used in a Phase 1 trial against NET in 2016.
combining drug screening platforms and patient-derived ex vivo cell cultures that mimic relevant aspects of the original tumors.
An autopsy study of the pancreas in people who died from unrelated causes discovered a remarkably high incidence of tiny asymptomatic NETs.
[104] As diagnostic imaging increases in sensitivity, such as endoscopic ultrasonography, very small, clinically insignificant NETs may be coincidentally discovered; being unrelated to symptoms, such neoplasms may not require surgical excision.