Neurofibromatosis type II
[3] There are two forms of the NF2:[4] Symptoms can occur at any age, typically in adolescence and early adulthood, and rarely seen in children, and the severity depends on the location of the tumours.
Symptoms include, but are not limited to:[citation needed] Because hearing loss in those with NF2 almost always occurs after acquisition of verbal language skills, people with NF2 do not always integrate well into Deaf culture and are more likely to resort to auditory assistive technology.
[citation needed] One of these devices is the cochlear implant, which can sometimes restore a high level of auditory function even when natural hearing is totally lost.
In these cases, an auditory brainstem implant (ABI) can restore some level of hearing, supplemented by lip reading.
[citation needed] Hearing loss may also result from benign tumors that grow on the vestibular and auditory nerves, which lead to the inner ear.
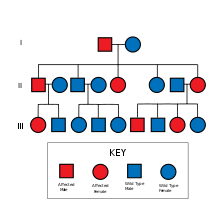
[citation needed] NF2 is caused by a defect in the gene that normally gives rise to a product called Merlin or Schwannomin, located on chromosome 22 band q11-13.1.
Recent studies showed that besides its cytoskeletal and cytoplasmic functions Merlin also translocates to the nucleus and suppresses proliferation by inhibiting E3 ubiquitin ligase CRL4(DCAF1).
[11][12] Mutations of NF2 is presumed to result in either a failure to synthesize Merlin or the production of a defective peptide that lacks the normal tumor-suppressive effect.
Loss of function mutations occurring in chromosome 22q, where Merlin proteins are coded, can promote tumorigenesis, or the creation of new tumorous cells.
They derive from the nerve sheaths of the upper part of the nervus vestibularis in the region between the central and peripheral myelin (Obersteiner-Redlich-Zone) within the area of the porus acousticus, 1 cm from the brainstem.
[citation needed] Many people with NF2 were included in studies that were designed to compare disease type and progression with exact determination of the associated mutation.
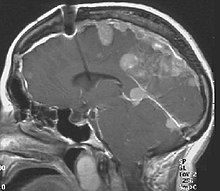
NF2 can be diagnosed due to the presence of a bilateral vestibular schwannoma, or an acoustic neuroma, which causes a hearing loss that may begin unilaterally.
This included the consideration of a LZTR1 mutation (schwannomatosis) instead of NF2 and excluded bilateral vestibular schwannomas that occur after 70 years of age.
Auditory canal decompression is another surgical technique that can prolong usable hearing when a vestibular schwannoma has grown too large to remove without damage to the cochlear nerve.
The bone overlying the acoustic nerve is removed, allowing the tumour to expand upward into the middle cranial fossa.
With conformal radiosurgical techniques, therapeutic radiation focused on the tumour, sparing exposure to surrounding normal tissues.
Auditory Brainstem Implants, or ABIs, are used when the cochlea or any portion of the cochleovestibular nerve are not functioning due to damage to those areas or anatomic abnormalities.
[24] The procedure is done by implanting a device that send an electrical signal directly to the cochlear nucleus, allowing sound to bypass the peripheral auditory system and straight into the brain stem.
It is a rare genetic disorder that involves noncancerous tumors of the nerves that transmit balance and sound impulses from the inner ear to the brain.
The prognosis is affected by early age onset, a higher number of meningiomas and schwannomas and having a decrease in mutation.