Peyronie's disease
Specifically, scar tissue forms in the tunica albuginea, the thick sheath of tissue surrounding the corpora cavernosa, causing pain, abnormal curvature, erectile dysfunction, indentation, loss of girth and shortening.
[4] The disease may cause pain; hardened, big, cord-like lesions (scar tissue known as "plaques"); or abnormal curvature of the penis when erect due to chronic inflammation of the tunica albuginea (CITA).
[8] Risk factors include diabetes mellitus, Dupuytren's contracture, plantar fibromatosis, penile trauma, smoking, excessive alcohol consumption, genetic predisposition, and European heritage.
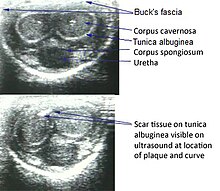
An ultrasound can provide conclusive evidence of Peyronie's disease, ruling out congenital curvature or other disorders.
[12] On penile ultrasonography, the typical appearance is hyperechoic focal thickening of the tunica albuginea.
Due to associated calcifications, the imaging of patients with Peyronie's disease shows acoustic shadowing, as illustrated in figures below.
Individuals with Peyronie's disease can present with erectile dysfunction, often related to venous leakage, due to insufficient drainage at the site of the plaque.
[23] Surgery such as the "Nesbit operation", which is named after Reed M. Nesbit (1898–1979), an American urologist at University of Michigan),[8] is considered a last resort and should only be performed by highly skilled urological surgeons knowledgeable in specialized corrective surgical techniques.
In 534 men undergoing routine prostate screening for cancer detection (without a specific urologic complaint), the prevalence of PD was 8.9 percent.