Spondylolysis
This leaves young athletes at increased risk, particularly when involved in repetitive hyperextension and rotation across the lumbar spine.
[4] Sports involving repetitive or forceful hyperextension of the spine, especially when combined with rotation are the main mechanism of injury for spondylolysis.
[3] Spondylolysis is a bony defect or fracture within the pars interarticularis of the vertebral arch in the spinal column.
When examining the vertebra, the pars interarticularis is the bony segment between the superior and inferior articular facet joints located anterior to the lamina and posterior to the pedicle.
The pars interarticularis is vulnerable to fracture during spinal hyperextension, especially when combined with rotation, or when experiencing a force during a landing.
[citation needed]X-rays (electromagnetic radiation) are projected through the body to produce an image of its internal structures.
If inconclusive a further CT scan can produce a 3-dimensional images to more clearly show the defect although the exam increases the patients radiation dose by at least an order of magnitude than plain x-rays.
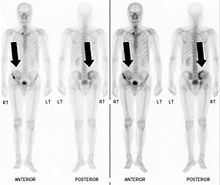
Bone scintigraphy combined with CT scan is considered the gold standard which means that it is best at detecting spondylolysis.
The duration of physical therapy a patient receives varies upon the severity of spondylolysis, however typically ranges from three to six months.
Once a patient completes physical therapy, and displays no symptoms or inflammation in the lower back, they are cleared to continue with daily or athletic activities.
However, a patient may need to maintain a variety of rehabilitation techniques after physical therapy to prevent the recurrence of spondylolysis.
Instead the local muscles in individuals with spondylolysis are vulnerable to dysfunction, which results in abnormal spinal stability causing chronic low back pain.
[18] In one study, patients are taught to train the co-contraction of deep abdominal muscles and lumbar multifidus in static postures, functional tasks and aerobic activities.
This is because motor programming eventually became automatic, and conscious control was no longer needed to contract the deep abdominal muscles during activities.
[18] Activity restriction of spondylolysis is advised for a short period of time once the patient becomes symptomatic, followed by a guided physical therapy program.
Once spondylolysis has been diagnosed, treatment often consists of a short rest period of two to three days, followed by a physical therapy program.
There should be restriction of heavy lifting, excessive bending, twisting and avoidance of any work, recreational activities or participation in sport that causes stress to the lumbar spine.
[19][21] Bracing immobilizes the spine in a flexed position for a short period to allow healing of the bony defect in the pars interarticularis.