Rotator cuff tear
[14] Epidemiological studies strongly support a relationship between age and cuff tear prevalence,[15][16][17] with the most common cause being age-related degeneration and, less frequently, sports injuries or trauma.
[20] People who play sports that involve overhead motions, such as swimming, water polo,[21] volleyball, baseball, and tennis, and American football quarterbacks are at a greater risk of experiencing a rotator cuff tear.
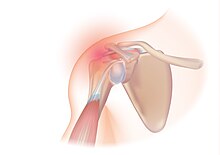
Another potential contributing cause is impingement syndrome, the most common non-sports related injury and which occurs when the tendons of the rotator cuff muscles become irritated and inflamed while passing through the subacromial space beneath the acromion.
[29][30] Well-documented anatomic factors include the morphologic characteristics of the acromion, a bony projection from the scapula that curves over the shoulder joint.
Environmental factors include age, shoulder overuse, smoking, and medical conditions that affect circulation or impair the inflammatory and healing response, such as diabetes mellitus.
[citation needed] Tendon transfers are prescribed for young, active cuff-tear individuals who experience weakness and decreased range of motion, but little pain.
Since pain arising from the neck is frequently 'referred' to the shoulder, the examination should include an assessment of the cervical spine looking for evidence suggestive of a pinched nerve, osteoarthritis, or rheumatoid arthritis.
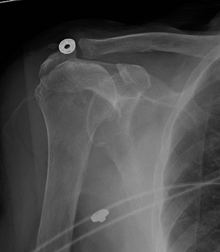
Double-contrast arthrography involves injecting contrast dye into the shoulder joint to detect leakage out of the injured rotator cuff,[36] and its value is influenced by the experience of the operator.
Furthermore, MRI enables the detection or exclusion of complete rotator cuff tears with reasonable accuracy and is also suitable for diagnosing other pathologies of the shoulder joint.
The role of X-ray, MRI, and ultrasound is adjunctive to clinical assessment and serves to confirm a diagnosis provisionally made by a thorough history and physical examination.
Acute injury is less frequent than chronic disease, but may follow bouts of forcefully raising the arm against resistance, as occurs in weightlifting, for example.
These traumatic tears predominantly affect the supraspinatus tendon or the rotator interval[37] and symptoms include severe pain that radiates through the arm, and limited range of motion, specifically during abduction of the shoulder.
[40] Chronic tears occur among individuals who constantly participate in overhead activities, such as pitching or swimming, but can also develop from shoulder tendinitis or rotator cuff disease.
[citation needed] Primary shoulder problems may cause pain over the deltoid muscle intensified by abduction against resistance – the impingement sign.
For impingement, these tests include the Hawkins-Kennedy impingement sign, in which an examiner medially rotates the injured individual's flexed arm, forcing the supraspinatus tendon against the coracoacromial ligament and so producing pain if the test is positive,[42] a positive painful arc sign, and weakness in external rotation with the arm at the side.
[48] An overall sensitivity of 91% (9% false negative rate) has been reported, indicating that magnetic resonance arthrography is reliable in the detection of partial-thickness rotator cuff tears.
[49] This modality can also reveal the presence of other conditions that may mimic rotator cuff tear at clinical examination, including tendinosis, calcific tendinitis, subacromial subdeltoid bursitis, greater tuberosity fracture, and adhesive capsulitis.
[50] However, MRI provides more information about adjacent structures in the shoulder, such as the capsule, glenoid labrum muscles, and bone, and these factors should be considered in each case when selecting the appropriate study.
Spurs may also be seen on the underside of the acromion, once thought to cause direct fraying of the rotator cuff from contact friction, a concept currently regarded as controversial.
[citation needed] As part of clinical decision-making, a simple, minimally invasive, in-office procedure, the rotator cuff impingement test, may be performed.
[citation needed] Shock wave therapy has seen widespread use since the 1990s to treat various musculoskeletal disorders including rotator cuff disease, but evidence of its efficacy remains dubious.
They found low to moderate certainty evidence, that there were very few clinically important benefits of shock wave therapy, and uncertainty regarding its safety.
Strain induced tendon remodeling, which is part of an accelerated rehabilitation protocol, has been shown to speed up the time to return to daily activities.
[61] Codman exercises (giant, pudding-stirring), to "permit the patient to abduct the arm by gravity, the supraspinatus remains relaxed, and no fulcrum is required" are widely used.
The use of NSAIDs, hot and cold packs, and physical therapy modalities, such as ultrasound, phonophoresis, or iontophoresis, can be instituted during this stretching period, if effective.
[61] This program involves a home therapy kit which includes elastic bands of six different colors and strengths, a pulley set, and a three-piece, one-meter-long stick.
[citation needed] The latest systematic reviews suggests (with low quality evidence) that total shoulder arthroplasty does not provide important benefits over hemiarthroplasty for glenohumeral osteoarthritis and rotator cuff tears.
[78] These include injecting an individual's own stem cells, growth factors or platelet rich plasma (PRP) into the repair site, and installing scaffolds as biological or synthetic supports to maintain tissue contour.
Gentle physical therapy guided motion is instituted at this phase, only to prevent stiffness of the shoulder; the rotator cuff remains fragile.
Based on examinations, they compile scores on tests; some examples are those created by the University of California at Los Angeles and the American Shoulder and Elbow Surgeons.