Trigeminal nerve
[4] Motor fibers pass through the trigeminal ganglion without synapsing on their way to peripheral muscles, their cell bodies being located in the nucleus of the fifth nerve, deep within the pons.
The trigeminal ganglion is analogous to the dorsal root ganglia of the spinal cord, which contain the cell bodies of incoming sensory fibers from the rest of the body.The ophthalmic, maxillary and mandibular branches leave the skull through three separate foramina: the superior orbital fissure, the foramen rotundum and the foramen ovale, respectively.
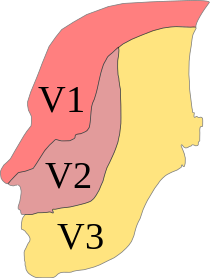
The ophthalmic nerve (V1) carries sensory information from the scalp and forehead, the upper eyelid, the conjunctiva and cornea of the eye, the nose (including the tip of the nose, except alae nasi), the nasal mucosa, the frontal sinuses and parts of the meninges (the dura and blood vessels).
The maxillary nerve (V2) carries sensory information from the lower eyelid and cheek, the nares and upper lip, the upper teeth and gums, the nasal mucosa, the palate and roof of the pharynx, the maxillary, ethmoid and sphenoid sinuses and parts of the meninges.
The injection of a local anesthetic, such as lidocaine, results in the complete loss of sensation from well-defined areas of the face and mouth.
The sensory function of the trigeminal nerve is to provide tactile, proprioceptive, and nociceptive afference to the face and mouth.
The trigeminal nerve carries general somatic afferent fibers (GSA), which innervate the skin of the face via ophthalmic (V1), maxillary (V2) and mandibular (V3) divisions.
The trigeminal nerve also carries special visceral efferent (SVE) axons, which innervate the muscles of mastication via the mandibular (V3) division.
With the exception of the tensor tympani, all these muscles are involved in biting, chewing and swallowing and all have bilateral cortical representation.
A unilateral central lesion (for example, a stroke), no matter how large, is unlikely to produce an observable deficit.
People without touch-position perception can feel the surface of their bodies and perceive touch in a broad sense, but they lack perceptual detail.
Sensory information is processed and modified at each level in the chain by interneurons and input from other areas of the nervous system.
From caudal to rostral (ascending from the medulla to the midbrain), they are the spinal trigeminal, the principal sensory and the mesencephalic nuclei.
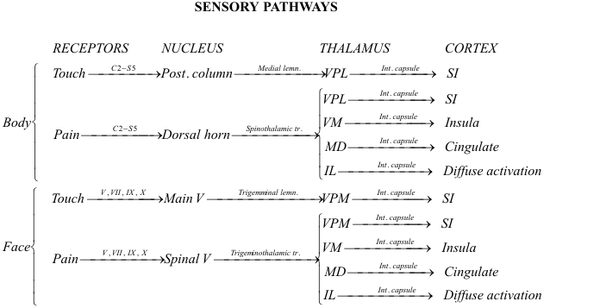
From the spinal trigeminal nucleus, secondary fibers cross the midline and ascend in the trigeminothalamic (quintothalamic) tract to the contralateral thalamus.
The present general understanding is that pain-temperature information from all areas of the human body is represented in the spinal cord and brainstem in an ascending, caudal-to-rostral fashion.
Information from the neck and the back of the head is represented in the cervical cord, and that from the face and mouth in the spinal trigeminal nucleus.
The lowest levels of the nucleus (in the upper cervical cord and lower medulla) represent peripheral areas of the face (the scalp, ears and chin).
The latter pathways are analogous to the spinomesencephalic and spinoreticular tracts of the spinal cord, which send pain-temperature information from the rest of the body to the same areas.
Fibers carrying touch-position information from the face and mouth via cranial nerves V, VII, IX, and X are sent to this nucleus when they enter the brainstem.
From the principal nucleus, secondary fibers cross the midline and ascend in the ventral trigeminothalamic tract to the contralateral thalamus.
The ventral trigeminothalamic tract runs parallel to the medial lemniscus, which carries touch-position information from the rest of the body to the thalamus.
Some sensory information from the teeth and jaws is sent from the principal nucleus to the ipsilateral thalamus via the small dorsal trigeminal tract.
Some of these incoming fibers go to the motor nucleus of the trigeminal nerve (V), bypassing the pathways for conscious perception.
Other incoming fibers from the teeth and jaws go to the main nucleus of V. This information is projected bilaterally to the thalamus and available for conscious perception.
They are automatic activities, requiring little conscious attention and involving a sensory component (feedback about touch-position) processed at the unconscious level in the mesencephalic nucleus.
With the exception of smell, all sensory input (touch-position, pain-temperature, sight, taste, hearing and balance) is sent to the thalamus and then the cortex.
Functional MRI imaging of a defined stimulus (for example, stroking the skin with a toothbrush) "lights up" a single focus in SI and two foci in SII.
Some pain-temperature fibers are sent to the medial dorsal thalamic nucleus (MD), which projects to the anterior cingulate cortex.
A stroke which cuts off the blood supply to this area (for example, a clot in the posterior inferior cerebellar artery) destroys both tracts simultaneously.
The result is a loss of pain-temperature (but not touch-position) sensation in a "checkerboard" pattern (ipsilateral face, contralateral body), facilitating diagnosis.