Anxiety
[6] It is often accompanied by muscular tension,[7] restlessness, fatigue, inability to catch one's breath, tightness in the abdominal region, nausea, and problems in concentration.
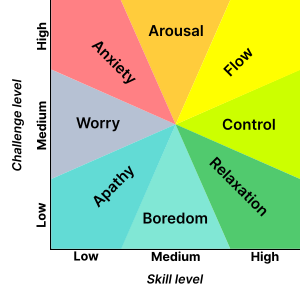
[18] In positive psychology, anxiety is described as the mental state that results from a difficult challenge for which the subject has insufficient coping skills.
[3][19] Fear and anxiety can be differentiated into four domains: (1) duration of emotional experience, (2) temporal focus, (3) specificity of the threat, and (4) motivated direction.
[20] Joseph E. LeDoux and Lisa Feldman Barrett have both sought to separate automatic threat responses from additional associated cognitive activity within anxiety.
[29] The cognitive effects of anxiety may include thoughts about suspected dangers, such as an irrational fear of dying or having a heart attack, when in reality all one is experiencing is mild chest pain, for example.
In Art and Artist (1932), the psychologist Otto Rank wrote that the psychological trauma of birth was the pre-eminent human symbol of existential anxiety and encompasses the creative person's simultaneous fear of – and desire for – separation, individuation, and differentiation.
Sweating, dizziness, headaches, racing heartbeats, nausea, fidgeting, uncontrollable crying or laughing and drumming on a desk are all common.
[41] The routine practice of slow, Device-Guided Breathing (DGB) is a major component of behavioral treatments for anxiety conditions.
Depending on the nature of the antecedent relations, cognitions, and situational factors, intergroup contact may be stressful and lead to feelings of anxiety.
[53][54][55] Additionally recent research has found that implicit racial evaluations (i.e. automatic prejudiced attitudes) can be amplified during intergroup interaction.
[65] Someone with panic disorder will eventually develop constant fear of another attack and as this progresses it will begin to affect daily functioning and an individual's general quality of life.
Some symptoms include: difficulty breathing, chest pain, dizziness, trembling or shaking, feeling faint, nausea, fear that you are losing control or are about to die.
[67][68] To be diagnosed, symptoms typically need to be present for at least six months, be more than would be expected for the situation, and decrease a person's ability to function in their daily lives.
[7][69] Other problems that may result in similar symptoms include hyperthyroidism, heart disease, caffeine, alcohol, or cannabis use, and withdrawal from certain drugs, among others.
[82] Specific measured 'environments' that have been associated with anxiety include child abuse, family history of mental health disorders, and poverty.
[86][87] Research upon adolescents who as infants had been highly apprehensive, vigilant, and fearful finds that their nucleus accumbens is more sensitive than that in other people when deciding to make an action that determined whether they received a reward.
As researchers note, "a sense of 'responsibility', or self-agency, in a context of uncertainty (probabilistic outcomes) drives the neural system underlying appetitive motivation (i.e., nucleus accumbens) more strongly in temperamentally inhibited than noninhibited adolescents".
[98][99] When investigating how anxiety is passed on from parents to children, it is important to account for sharing of genes as well as environments, for example using the intergenerational children-of-twins design.
These investigations were based on hypotheses about how certain known genes influence neurotransmitters (such as serotonin and norepinephrine) and hormones (such as cortisol) that are implicated in anxiety.
[102] The reason that most candidate gene findings have not replicated is that anxiety is a complex trait that is influenced by many genomic variants, each of which has a small effect on its own.
[134] Cognitive distortions such as overgeneralizing, catastrophizing, mind reading, emotional reasoning, binocular trick, and mental filter can result in anxiety.
Psychodynamic theory posits that anxiety is often the result of opposing unconscious wishes or fears that manifest via maladaptive defense mechanisms (such as suppression, repression, anticipation, regression, somatization, passive aggression, dissociation) that develop to adapt to problems with early objects (e.g., caregivers) and empathic failures in childhood.
[137] When people are confronted with unpleasant and potentially harmful stimuli such as foul odors or tastes, PET-scans show increased blood flow in the amygdala.
Social risk factors for anxiety include a history of trauma (e.g., physical, sexual or emotional abuse or assault), bullying, early life experiences and parenting factors (e.g., rejection, lack of warmth, high hostility, harsh discipline, high parental negative affect, anxious childrearing, modelling of dysfunctional and drug-abusing behaviour, discouragement of emotions, poor socialization, poor attachment, and child abuse and neglect), cultural factors (e.g., stoic families/cultures, persecuted minorities including those with disabilities), and socioeconomics (e.g., uneducated, unemployed, impoverished although developed countries have higher rates of anxiety disorders than developing countries).
[140] A 2019 comprehensive systematic review of over 50 studies showed that food insecurity in the United States is strongly associated with depression, anxiety, and sleep disorders.
In particular, learning mastery (the degree to which people perceive their lives to be under their own control) and instrumentality, which includes such traits as self-confidence, self-efficacy, independence, and competitiveness fully mediate the relation between gender and anxiety.
[142] The first step in the management of a person with anxiety symptoms involves evaluating the possible presence of an underlying medical cause, the recognition of which is essential in order to decide the correct treatment.
A 2017 review found that psychological or educational interventions have a small yet statistically significant benefit for the prevention of anxiety in varied population types.
[156] In the central nervous system (CNS), the major mediators of the symptoms of anxiety disorders appear to be norepinephrine, serotonin, dopamine, and gamma-aminobutyric acid (GABA).
Increased flow in the right parahippocampal region and reduced serotonin type 1A receptor binding in the anterior and posterior cingulate and raphe of patients are the diagnostic factors for prevalence of anxiety disorder.