Cardiopulmonary resuscitation
The objective is to delay tissue death and to extend the brief window of opportunity for a successful resuscitation without permanent brain damage.
[17][18] As a general reference, the recommended order (according to the guidelines of many related associations as AHA and Red Cross) is: If there are multiple rescuers, these tasks can be distributed and performed simultaneously to save time.
[25]The patient's head is commonly tilted back (a head-tilt and chin-lift position) for improving the air flow if ventilations can be used.
[32] There exist some plastic shields and respirators that can be used in the rescue breaths between the mouths of the rescuer and the victim, with the purposes of sealing a better vacuum and avoiding infections.
The common model of defibrillator (the AED) is an automatic portable machine that guides to the user with recorded voice instructions along the process, and analyzes the victim, and applies the correct shocks if they are needed.
Many official guides recommend continuing a cardiopulmonary resuscitation until emergency medical services arrive (for trying to keep the patient alive, at least).
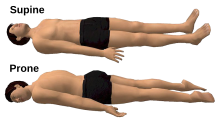
[48] During pregnancy when a woman is lying on her back, the uterus may compress the inferior vena cava and thus decrease venous return.
Also, it is not indicated in asystole or pulseless electrical activity (PEA), in those cases a normal CPR would be used to oxygenate the brain until the heart function can be restored.
All these tasks (calling by phone, getting an AED, and the chest compressions and rescue breaths maneuvers of CPR) can be distributed between many rescuers who make them simultaneously.
This depends on the amount of water, but it is convenient to avoid starting the defibrillation on a floor with puddles, and to dry the wet areas of the patient before (fast, even with any cloth, if that could be enough).
[56] Timing devices can feature a metronome (an item carried by many ambulance crews) to assist the rescuer in achieving the correct rate.
[71] However the disadvantages are cost to purchase, time to train emergency personnel to use them, interruption to CPR to implement, potential for incorrect application and the need for multiple device sizes.
[78] As a result, the Red Cross updated and endorsed its emergency preparedness application, which uses pictures, text and videos to assist the user.
Even in the case of a "non-shockable" rhythm, such as pulseless electrical activity (PEA) where defibrillation is not indicated, effective CPR is no less important.
[81] Studies have shown that immediate CPR followed by defibrillation within 3–5 minutes of sudden VF cardiac arrest dramatically improves survival.
CARES reports CPR results from a catchment area of 115 million people, including 23 state-wide registries, and individual communities in 18 other states as of 2019.
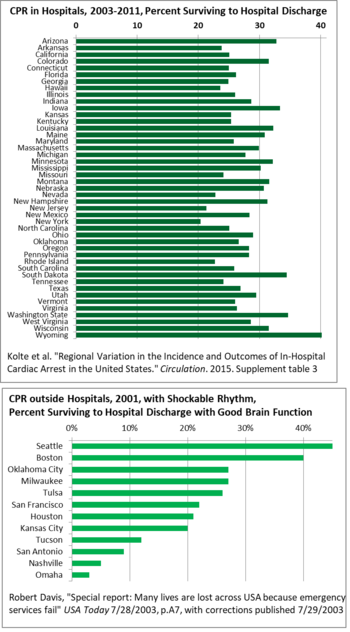
[100] Geographically, there is wide variation state-to-state in survival after CPR in US hospitals, from 40% in Wyoming to 20% in New York, so there is room for good practices to spread, raising the averages.
[144] A major reason for the variation has been delay in some areas between the call to emergency services and the departure of medics, and then arrival and treatment.
[152][153] One study found that members of the public having received CPR training in the past lack the skills and confidence needed to save lives.
[148][155] Bystanders more commonly administer CPR when in public than when at the person's home, although health care professionals are responsible for more than half of out-of-hospital resuscitation attempts.
[38][157] The first formal study into gender bias in receiving CPR from the public versus professionals was conducted by the American Heart Association and the National Institutes of Health (NIH), and examined nearly 20,000 cases across the U.S.
The study found that women are six percent less likely than men to receive bystander CPR when in cardiac arrest in a public place, citing the disparity as "likely due to the fear of being falsely accused of sexual assault.
New research is currently needed to determine what role CPR, defibrillation, and new advanced gradual resuscitation techniques will have with this new knowledge.
[163] CPR is often severely misrepresented in movies and television as being highly effective in resuscitating a person who is not breathing and has no circulation.
[164] When educated on the actual survival rates, the proportion of patients over 60 years of age desiring CPR should they have a cardiac arrest drops from 41% to 22%.
This action would deliver a controlled flow of air into the patient's lungs, aiding in oxygenation and facilitating the exchange of gases.
The combination was first seen in a 1962 training video called "The Pulse of Life" created by James Jude, Guy Knickerbocker, and Peter Safar.
[181] Their combined findings were presented at the annual Maryland Medical Society meeting on September 16, 1960, in Ocean City, and gained widespread acceptance over the following decade, helped by the video and speaking tour they undertook.
[183] CPR methods continued to advance, with developments in the 2010s including an emphasis on constant, rapid heart stimulation, and a de-emphasis on the respiration aspect.
Studies have shown that people who had rapid, constant heart-only chest compression are 22% more likely to survive than those receiving conventional CPR that included breathing.