Chronic pulmonary aspergillosis
Chronic pulmonary aspergillosis is a long-term fungal infection caused by members of the genus Aspergillus—most commonly Aspergillus fumigatus.
[8] The term describes several disease presentations with considerable overlap, ranging from an aspergilloma[12]—a clump of Aspergillus mold in the lungs—through to a subacute, invasive form known as chronic necrotizing pulmonary aspergillosis which affects people whose immune system is weakened.
If there is a single, stable cavity that provides minimal symptoms, the term 'simple aspergilloma' is commonly used to distinguish it from more severe forms of chronic pulmonary aspergillosis.
[16] In contrast to aspergilloma and Aspergillus nodules, the vast majority of people with chronic cavitary pulmonary aspergillosis have positive tests for IgG antibodies.
[8][6] In contrast to chronic cavitary pulmonary aspergillosis, for example, IgG antibodies for Aspergillus or an antigen called galactomannan may be found in the blood as well as in sputum samples.
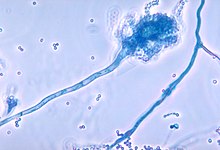
The vast majority of cases are caused by Aspergillus fumigatus—a filamentous fungus found ubiquitously on every continent including Antarctica.
[28] It is postulated that conidia, once inhaled, are attacked by the host immune defences—specifically phagocytes and alveolar macrophage resident in the small airways.
It is unknown whether these defences are sufficient to clear conidia or whether they are directly responsible for the inflammation leading to chronic pulmonary aspergillosis.
Some Aspergillus have the ability to inhibit phagocyte nicotinamide adenine dinucleotide phosphate oxidase activation which is one of the core defence systems against filamentous fungi, which may increase susceptibility of the host to chronic pulmonary aspergillosis.
[29] The diagnosis of chronic pulmonary aspergillosis is often initially considered when patients present with a history of unintentional weight loss and fatigue.
Confirmation of this suspicion is normally achieved with a combination of radiological imaging and serological testing, with the goal of excluding other diagnoses like tuberculosis and finding evidence of fungus present.
Whilst cavities seen on chest X-rays can raise suspicion, positive IgG testing for Aspergillus is required for confirmation.
[30] The distinction between simple aspergilloma, and more advanced chronic cavitary pulmonary aspergillosis, will depend on the severity of inflammation, radiological evidence, and changes over time.
This must be accompanied by at least one symptom of fever, weight loss, fatigue, cough, sputum production, haemoptysis or shortness of breath for at least 3 months.