Colorectal cancer
The common theme among these genes, across both tumor types, is their involvement in Wnt and TGF-β signaling pathways, which results in increased activity of MYC, a central player in colorectal cancer.
[56] Consequently, a deficiency in MMR proteins may lead to an inability to detect and repair genetic damage, allowing for further cancer-causing mutations to occur and colorectal cancer to progress.
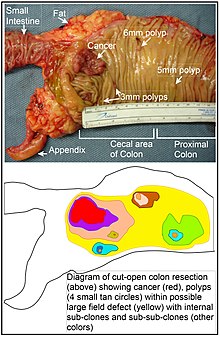
[63][64] However, as pointed out by Rubin, "The vast majority of studies in cancer research has been done on well-defined tumors in vivo, or on discrete neoplastic foci in vitro.
"[65][66] Similarly, Vogelstein et al.[67] pointed out that more than half of somatic mutations identified in tumors occurred in a pre-neoplastic phase (in a field defect), during growth of apparently normal cells.
A combinatorial therapeutic approach based on the previously introduced consensus molecular subtypes (CMSs) and EpiCs could significantly enhance current treatment strategies.
[81] Colorectal cancer diagnosis is performed by sampling areas of the colon suspicious for possible tumor development, typically during colonoscopy or sigmoidoscopy, depending on the location of the lesion.
[91] Increasing surveillance, engaging in physical activity, consuming a diet high in fiber, quitting smoking and limiting alcohol consumption decrease the risk.
[94][95][96] The risk of colon cancer can be reduced by maintaining a normal body weight through a combination of sufficient exercise and eating a healthy diet.
[99]: 432–433 [100]: 125–126 In 2018 the National Cancer Institute stated that "There is no reliable evidence that a diet started in adulthood that is low in fat and meat and high in fiber, fruits, and vegetables reduces the risk of CRC by a clinically important degree.
[123] However, research in the UK has found that for these immunochemical tests, the threshold for further investigation is set at a point that may miss more than half of bowel cancer cases.
The research suggests that the NHS England's Bowel Cancer Screening Programme could make better use of the test's ability to provide the exact concentration of blood in faeces (rather than only whether it is above or below a cutoff level).
[138] The UK Bowel Cancer Screening Programme aims to find warning signs in people aged 60 to 74, by recommending a faecal immunochemical test (FIT) every two years.
However, when it is detected at later stages (for which metastases are present), this is less likely and treatment is often directed at palliation, to relieve symptoms caused by the tumour and keep the person as comfortable as possible.
[142] For people with localized cancer, the preferred treatment is complete surgical removal with adequate margins, with the attempt of achieving a cure.
[148] Another class of drugs used in the second line setting are epidermal growth factor receptor inhibitors, of which the three FDA approved ones are aflibercept, cetuximab and panitumumab.
[154] While a combination of radiation and chemotherapy may be useful for rectal cancer,[20] for some people requiring treatment, chemoradiotherapy can increase acute treatment-related toxicity and has not been shown to improve survival rates compared to radiotherapy alone, although it is associated with less local recurrence.
[143] For squamous cell carcinoma of the anal canal, chemoradiation therapy (CRT) with 5-FU and mitomycin C is preferred over radiation alone, offering improved survival outcomes but with increased risks of acute hematological toxicity.
[162] On the other hand, in a prospective phase 2 study published in June 2022 in The New England Journal of Medicine, 12 patients with Deficient Mismatch Repair (dMMR) stage II or III rectal adenocarcinoma were administered single-agent dostarlimab, an anti–PD-1 monoclonal antibody, every three weeks for six months.
Colorectal cancer is highly stigmatized and can elicit feelings of disgust from patients, healthcare professionals, families, intimate partners, and the general public.
[176] Face-to-face interventions such as clinician-patient talk therapy, body-mind-spirit practices, and support group sessions have been identified as most effective in reducing anxiety and depression in CRC patients.
A CT-scan of the chest, abdomen, and pelvis can be considered annually for the first 3 years for people who are at high risk of recurrence (for example, those who had poorly differentiated tumors or venous or lymphatic invasion) and are candidates for curative surgery (with the aim to cure).
[180][181] For people who have undergone curative surgery or adjuvant therapy (or both) to treat non-metastatic colorectal cancer, intense surveillance and close follow-up have not been shown to provide additional survival benefits.
People with tumors that lacked CTNNB1 expression (β-catenin), involved in Wnt signalling pathway, required more than 18 Metabolic equivalent (MET) hours per week, a measure of exercise, to observe a reduction in colorectal cancer mortality.
In clinical studies, a pro-inflammatory response was found in people with stage II-III colorectal cancer who underwent 2 weeks of moderate exercise after completing their primary therapy.
The constitutive activation of PI3K/AKT/mTOR pathway may explain the loss of p27 and excess energy balance may up-regulate p27 to stop cancer cells from dividing.
[188] Whilst the impact of colorectal cancer on those who survive varies greatly there will often be a need to adapt to both physical and psychological outcomes of the illness and its treatment.
[196] For example, it is common for people to experience incontinence,[197] sexual dysfunction,[198] problems with stoma care[199] and fear of cancer recurrence[200] after primary treatment has concluded.
A qualitative systematic review published in 2021 highlighted that there are three main factors influencing adaptation to living with and beyond colorectal cancer: support mechanisms, severity of late effects of treatment, and psychosocial adjustment.
[179][211] Instances of EOCC have increased over the last decade, specifically in patient populations aged 20 to 40 years old throughout North America, Europe, Australia, and China.
[179][211][212] While advancements in the diagnostic procedure may have some impact, reduced likelihood of screening among these populations suggests detection bias is not a major contributor to this trend.