Discovery and development of phosphodiesterase 5 inhibitors
[1] Phosphodiesterase 5 (PDE5) is widely expressed in several tissues in the body for example brain, lung, kidney, urinary bladder, smooth muscle and platelets.
[2] The therapeutic effects of PDE5 inhibition have been demonstrated in several cardiovascular conditions, chronic kidney disease and diabetes mellitus.
[3] The human genome contains at least 21 genes involved in determining the intracellular levels of cAMP and cGMP by the expression of phosphodiesterase proteins or PDE's.
[10] In humans the distribution of PDE5A1 and PDE5A2 isoforms is the same and can be found in the brain, lung tissue, heart, liver, kidneys, bladder, prostate, urethra, penis, uterus and skeletal muscles.
[9] The active site is a deep pocket at the junction of the 3 subdomains and is lined with highly conserved residues between isotypes of PDE.
[17] Upregulation of PDE5 gene expression has been observed in animal models of pulmonary hypertension, and is thought to contribute to vasoconstriction in the lung.
[9] As of 2011, the long-acting agent tadalafil is licensed for the treatment of urinary symptoms resulting from benign prostatic hyperplasia.
[3] PDE5 inhibitors have shown promise in the treatment of heart failure with reduced ejection fraction through several beneficial effects on lung vasculature, cardiac remodelling and diastolic function.
[3] A study showed that effective treatment of pulmonary arterial hypertension with sildenafil improved functional capacity and reduced right ventricular mass in patients.
The effects on right ventricular remodeling were significantly greater in comparison with the non-selective endothelial receptor antagonist bosentan.
[7] However, PDE5 inhibitors may be harmful in patients with heart failure with preserved ejection fraction due to potential negative inotropic effects.
[3] Experimental studies in animals have shown that PDE5 inhibitors may reverse kidney damage independently of their effects on blood pressure through intra-renal mechanisms.
[3] Sildenafil has been shown to be at least as effective as calcium channel blockers in treating severe Raynaud's phenomenon (RP) associated with systemic sclerosis and digital ulceration.
[3] Sildenafil has been shown to significantly improve neurovascular coupling without affecting overall cerebral blood flow by increasing brain levels of cGMP, evoking neurogenesis and reducing neurological deficits in rats 2 or 24 hours after stroke.
[3] Adding PDE5 inhibitors to SSRI drugs (e.g. paroxetine) for the treatment of premature ejaculation could result in better ejaculatory control according to recent studies.
Increased levels of cGMP have been shown to occur in human-cultured vaginal smooth muscle cells treated with a PDE5 inhibitor suggesting involvement of the NO/cGMP axis in the female sexual response.
[21] Many tissues contain PDE5, such as lungs, kidneys, brain, platelets, liver, prostate, urethra, bladder and smooth muscles.
Because of the localization of PDE5 in the smooth muscle tissue, inhibitors were developed for the treatment of erectile dysfunction along with pulmonary hypertension.
It was the result of extensive research on chemical agents targeting PDE5 that could be effective in treatment of coronary heart disease.
These drugs came out of research programs focusing on finding PDE5 inhibitors for the treatment of cardiovascular diseases and erectile dysfunction.
[24] Because of severe adverse effects and patients dissatisfaction with current therapy choices other inhibitors have recently been approved for clinical use.
[27] Erection is triggered by release of the neurotransmitter nitric oxide (NO) from non-adrenergic and non-cholinergic neurons from nerve ending in the penis as well as from endothelial cells.
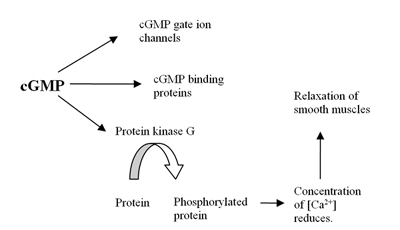
NO activates soluble guanylyl cyclase in smooth muscle cells in the penis which results in increased production of 3'-5'-cyclic guanosine monophosphate from guanosine-5'-triphosphate (GTP).
[34] Conformational change occurs when cGMP binds to the allosteric site that exposes serine and permits phosphorylation.
The difference of the molecular structures is the reason for interaction with the catalytic site of PDE5 and improves the affinity of these compounds compared with cGMP selectivity.
[33] The pharmacophore model of PDE5 usually consists of one hydrogen bond acceptor, one hydrophobic aliphatic carbon chain and two aromatic rings.
PDE5 inhibitors are generally well tolerated, with side effects including transient headaches, flushing, dyspepsia, congestion and dizziness.
[3] There have also been reports of temporary vision disturbances with sildenafil and, to a lesser extent, vardenafil, and back and muscle pain with tadalafil.
[3] Several reports are about approaches to improve PDE5 inhibitors, where as chemical groups have been switched out to increase potency and selectivity, which should potentially lead to drugs with fewer side effects.








|
|
This caption uses
trivial wording
.
(
July 2017
)
|

|
|
This caption uses
trivial wording
.
(
July 2017
)
|

|
|
This caption uses
trivial wording
.
(
July 2017
)
|